The Diagnostic Steps to Classify Azoospermia
Before planning any surgical sperm retrieval procedure, a structured clinical evaluation is essential. This diagnostic roadmap allows us to confirm the diagnosis definitively and accurately classify the type of azoospermia, ensuring you receive the most targeted treatment approach.
1. Definitive Confirmation of Azoospermia
The Protocol: Two separate semen analyses, each including a meticulous examination of a centrifuged pellet.
Why It Matters: This step is mandatory to rule out severe oligospermia (an extremely low sperm count). Without high-speed centrifugation, rare sperm cells can easily be missed, leading to a misdiagnosis of complete azoospermia.
2. Comprehensive Hormonal Profile
The Protocol: Blood tests to evaluate key reproductive hormones, including FSH (Follicle-Stimulating Hormone), LH (Luteinizing Hormone), Testosterone, and Prolactin.
Why It Matters: Hormonal balance acts as a window into testicular function. For instance, significantly elevated FSH levels strongly point toward testicular production failure (Non-Obstructive Azoospermia or NOA). Conversely, normal FSH levels coupled with low semen volume frequently suggest a physical blockage, such as an ejaculatory duct obstruction.
3. Advanced Genetic Testing
The Protocol: Peripheral blood analysis for Karyotyping (chromosome analysis) and Y-chromosome microdeletion screening.
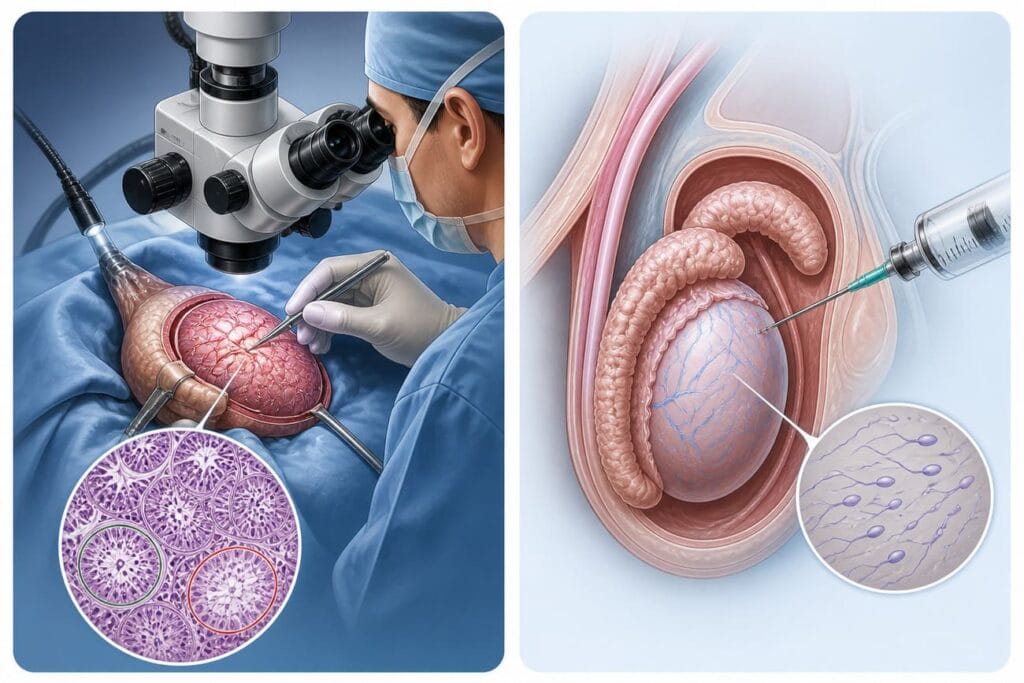
Why It Matters: Identifying the underlying genetic blueprint is crucial before selecting a surgical path. Specifically, microdeletions in the AZFa or AZFb regions carry a near-zero prognosis for successful sperm recovery. Knowing this information beforehand protects couples from undergoing unnecessary, invasive surgeries like micro-TESE when the biological probability is absent.
4. Testicular Volume Assessment
The Protocol: A detailed transscrotal ultrasound evaluation.
Why It Matters: Physical dimensions correlate directly with production capacity. A small testicular volume (typically <12 mL) heavily suggests reduced baseline production (NOA). On the other hand, normal testicular volume paired with normal FSH levels strongly favors an obstructive framework (Obstructive Azoospermia or OA).
5. CBAVD and Cystic Fibrosis Screening
The Protocol: Clinical examination of the scrotum, followed by CFTR gene mutation testing if the vas deferens cannot be palpated on both sides.
Why It Matters: Congenital Bilateral Absence of the Vas Deferens (CBAVD) is a known variant (forme fruste) of Cystic Fibrosis. If CBAVD is identified, screening both partners for CFTR mutations is absolutely vital to understand and manage any genetic transmission risks before proceeding with assisted reproduction.