PCOD and PCOS Treatment in Ahmedabad— A Stepped, Science-Based Approach
We want to say something clearly, right at the start: PCOD and PCOS are among the most treatable causes of infertility. The majority of women who come to Wellspring IVF & Women's Hospital in Ahmedabad with a PCOS diagnosis do not need IVF. Many do not even need advanced medication. What they need is the right diagnosis, the right lifestyle guidance, and — if fertility is the goal — a carefully sequenced treatment protocol that gives the least invasive approach the full chance it deserves before anything more complex is considered.
That is the philosophy Dr. Pranay Shah has practised for 15 years. It is called a Stepped Care Approach, and it is the reason so many women leave our clinic not just pregnant — but genuinely informed about their own bodies.
PCOD and PCOS Treatment — At a Glance
PCOD and PCOS Treatment — At a Glance
| Parameter | Details |
|---|---|
| Condition | PCOD and PCOS (Polycystic Ovarian Disease or Syndrome) |
| Primary Cause | Hormonal Imbalance — Excess Androgens + Insulin Resistance |
| First-Line Treatment | Lifestyle Modification + Metformin (NOT IVF) |
| Ovulation Induction | Letrozole or Clomiphene — most patients respond within 3 cycles |
| IVF Required? | Only when ovulation induction fails — the last step, not the first |
| Pregnancy Possible? | Yes. With correct stepped care, most PCOS patients conceive naturally or with minimal intervention |
| Specialist | Dr. Pranay Shah — 15+ Years Experience | PCOS Fertility Expert |
| Consultation |  9099946050 | Second Opinion Available 9099946050 | Second Opinion Available |
What Is PCOD and PCOS? Understanding the Condition Before the Treatment
PCOD (Polycystic Ovarian Disease) and PCOS (Polycystic Ovarian Syndrome) are related hormonal conditions that affect the way a woman’s ovaries function. Although the names are often used interchangeably, there is a subtle difference: PCOD is generally considered a milder, more common condition where the ovaries produce many partially matured eggs that accumulate as small cysts. PCOS is a broader metabolic and endocrine disorder with more complex hormonal disruption.
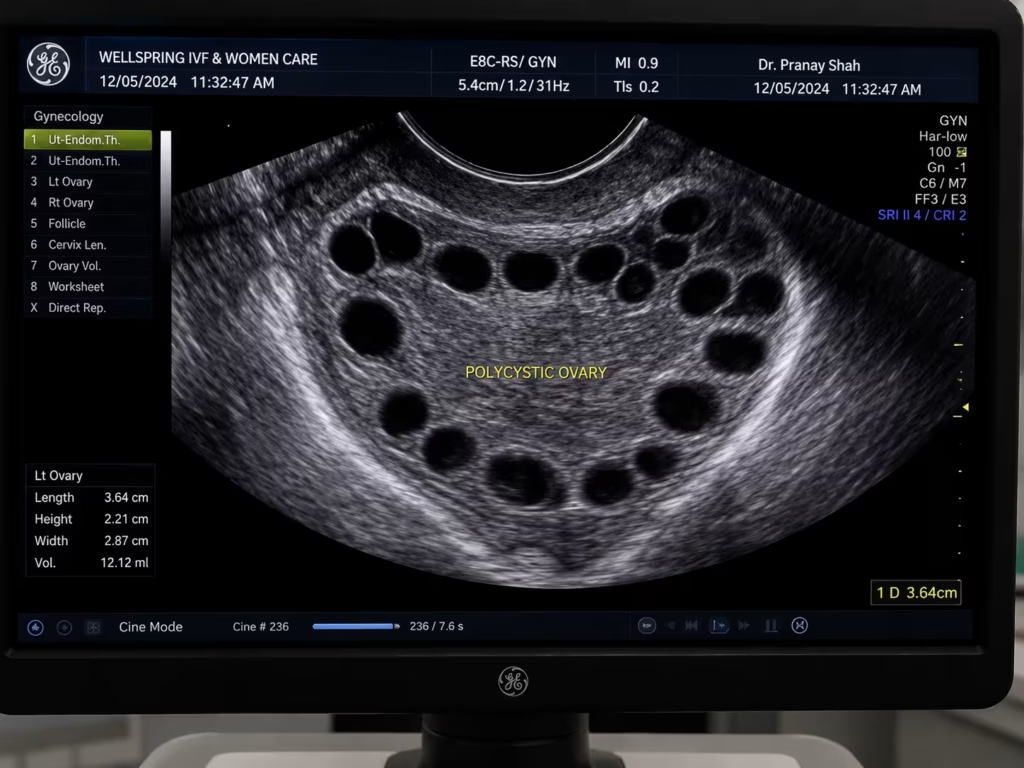
In both conditions, the ovaries produce excess androgens (male hormones like testosterone), which interferes with the normal process of ovulation. Rather than one mature egg being released each month, eggs remain trapped in follicles, causing the characteristic ‘string of pearls’ appearance on an ultrasound scan.
The root hormonal driver in most PCOS cases is insulin resistance. When the body’s cells do not respond efficiently to insulin, the pancreas produces more of it. Excess insulin then signals the ovaries to produce more androgens, creating a cycle that disrupts ovulation, metabolism, skin, hair, and mood simultaneously.
“PCOS is not just a fertility problem — it is a metabolic condition that affects the whole body. In my 15 years of treating PCOS patients in Ahmedabad, I have seen that when we address the root cause — insulin resistance, hormonal balance, and lifestyle — the ovaries often regulate themselves. We do not need to rush to IVF. We need to give the body what it is missing, in the right sequence.”
– Dr. Pranay Shah, MS (ObGy), Director, Wellspring IVF & Women’s Hospital
Common Symptoms of PCOD and PCOS
PCOS and PCOD present differently in different women. Some experience obvious, disruptive symptoms from their teens. Others have very subtle signs that only become apparent when they are trying to conceive. The most common symptoms include:
- Irregular or absent periods: cycles that are longer than 35 days, highly unpredictable, or absent for months.
- Unexplained weight gain: particularly around the abdomen, driven by insulin resistance rather than diet alone.
- Acne and oily skin: caused by elevated androgen levels stimulating excess sebum production.
- Hirsutism (excess facial or body hair): fine hair appearing on the chin, upper lip, chest, or abdomen.
- Hair thinning or scalp hair loss: androgenic alopecia pattern, similar to male-pattern thinning.
- Mood changes, anxiety, or depression: linked to hormonal fluctuations and the psychological burden of managing chronic symptoms.
- Fatigue: related to poor glucose metabolism and disrupted sleep.
- Difficulty conceiving: due to absent or infrequent ovulation — the primary fertility impact of PCOS.
You do not need to have all of these symptoms to have PCOS. A diagnosis is typically confirmed by the Rotterdam Criteria — the presence of at least two of three features: irregular ovulation, elevated androgen levels, and polycystic ovaries on ultrasound.
Watch Our Video on PCOS/PCOD/PMOS and Weight loss difficulty
Learn why weight loss becomes difficult in PCOS/PCOD and how hormonal and metabolic factors affect body weight.
What You Will Learn
Understand the connection between PCOS, insulin resistance, and weight management.
- PCOS and weight gain explained
- Insulin resistance and metabolism
- Common weight loss challenges
- Effective lifestyle and treatment strategies
The Wellspring Stepped Care Approach for PCOD and PCOS
Lifestyle Modification — The Foundation of PCOS Management
For many women with PCOS, particularly those who are overweight or insulin-resistant, targeted lifestyle changes produce results that no medication can match. This is not a generic ‘eat healthy and exercise’ directive — it is a structured protocol.
- Targeted weight reduction of 5–10% of body weight, which can spontaneously restore ovulation in many PCOS patients without any medication.
- Low-GI dietary modifications that reduce insulin spikes — shifting the body’s metabolic environment to support regular ovulation.
- Structured daily physical activity — 30–45 minutes of moderate exercise proven to improve insulin sensitivity and hormone profiles.
- Stress reduction techniques — cortisol is a significant disruptor of the HPO (hypothalamic-pituitary-ovarian) axis and worsens PCOS symptoms.
Metformin — Targeting the Root Cause (Insulin Resistance)
Where lifestyle changes alone are insufficient, particularly in patients with confirmed insulin resistance or elevated fasting insulin, we introduce Metformin. This is a medication familiar from diabetes management, but in PCOS it works by improving the body’s sensitivity to insulin — which reduces androgen production and often restores ovulation.
- Metformin reduces circulating insulin levels, which in turn lowers androgen production from the ovaries.
- It supports weight loss in insulin-resistant patients, making lifestyle changes more effective.
- It can improve menstrual regularity and, in some women, restore spontaneous ovulation.
Ovulation Induction — Letrozole or Clomiphene (For Fertility)
For patients whose goal is pregnancy and who are not ovulating on lifestyle and Metformin alone, the next step is ovulation induction. This is a simple, non-invasive oral medication protocol that stimulates the ovaries to develop and release one healthy egg per cycle.
Letrozole (our first choice for PCOS)
Current evidence strongly supports Letrozole as the preferred ovulation induction agent in PCOS over Clomiphene. It produces a more physiological hormone response, with better endometrial lining development and higher live birth rates per cycle in PCOS patients.
Clomiphene Citrate
Remains a valid option in specific clinical situations. It works by blocking oestrogen receptors in the brain, triggering a hormonal cascade that stimulates egg development.
All ovulation induction cycles at Wellspring are carefully monitored with serial ultrasound scans to track follicle development and time intercourse or IUI optimally.
IUI — Intrauterine Insemination (If Ovulation Induction Alone Is Insufficient)
If ovulation induction is successful (confirmed egg release) but pregnancy has not occurred after 3–4 monitored cycles, we consider adding IUI Treatment to the protocol. In IUI, a processed and concentrated sperm sample is placed directly into the uterus at the confirmed time of ovulation, increasing the probability of fertilisation.
IVF — Only When Clinically Justified
IVF is recommended for PCOS patients only when the above steps have been given a genuine clinical trial and have not resulted in pregnancy. Specific situations where IVF becomes the appropriate next step include:
- Confirmed tubal factor alongside PCOS — IUI cannot bypass this barrier.
- Significant male factor infertility present simultaneously.
- Age above 35 with declining ovarian reserve.
- Resistance to 6+ cycles of ovulation induction.
Note: At Wellspring, we frequently recommend a Freeze-All approach for PCOS patients to significantly reduce OHSS risk while maintaining excellent outcomes.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

DUrmi Chauhan
How PCOD and PCOS Specifically Affects Your Fertility
The primary fertility impact of PCOS is anovulation — the absence of regular ovulation. Without a released egg, pregnancy is not possible in a natural cycle.
However, it is important to understand that PCOS patients typically have a normal or even high number of antral follicles and a good ovarian reserve.
The problem is not egg quantity — it is the hormonal environment preventing those eggs from maturing and releasing. This is genuinely good news. It means that once the hormonal disruption is corrected — whether through lifestyle, medication, or assisted reproduction — the underlying egg reserve is often healthy and responsive.
Many of our PCOS patients who were deeply concerned about their fertility have achieved pregnancy with relatively simple, low-cost interventions.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Related Fertility Conditions We Commonly See Alongside PCOS
PCOS sometimes co-exists with other conditions that require separate evaluation and management. At Wellspring IVF, a comprehensive diagnostic workup ensures nothing is missed:
- Endometriosis — can co-exist with PCOS and requires separate laparoscopic assessment.
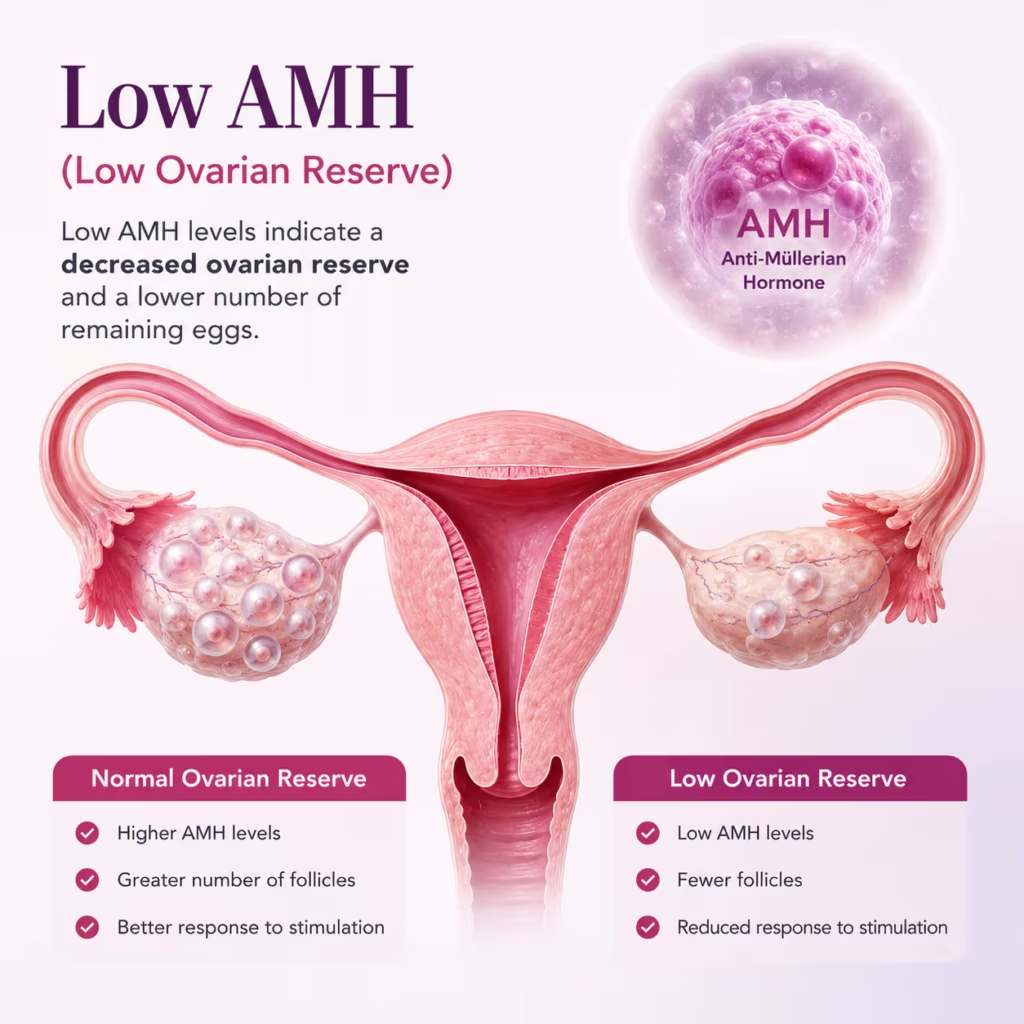
- Low AMH and Poor Ovarian Reserve — though less common in PCOS patients, it can occur, particularly after 35.
- Uterine Fibroids — may be found incidentally during PCOS evaluation ultrasound.
- Blocked Fallopian Tubes — important to rule out before initiating ovulation induction, as it changes the treatment pathway.
- Male Factor Infertility — a semen analysis is part of our first-visit evaluation. We also evaluate for conditions like Azoospermia and Oligospermia.
Why Women in Ahmedabad Trust Dr. Pranay Shah for PCOS Treatment
Dr. Pranay Shah has treated hundreds of PCOS patients across the spectrum — from young women managing symptoms to couples in their mid-30s who have been trying to conceive for years. His approach is defined by three principles that are often missing in routine fertility care:
Genuine Diagnostic Depth
Not all PCOS is the same. Dr. Shah reviews your full hormonal panel before making any treatment recommendation.
Respect for the Stepped Care Sequence
We do not skip steps. We will only recommend IVF when it is the medically appropriate next step.
Clear Communication at Every Step
Every patient at Wellspring leaves their consultation understanding their diagnosis, the reasoning behind each treatment recommendation, and the realistic probability of success.
Frequently Asked Questions
Are PCOD and PCOS the same condition?
They are related but not identical. PCOD typically refers to a milder hormonal imbalance where multiple immature follicles accumulate in the ovaries. PCOS is a broader metabolic and endocrine disorder with more pronounced hormonal disruption. Both are treatable.
Can I get pregnant naturally with PCOS?
Yes — and many women do. PCOS causes infrequent or absent ovulation, but it does not prevent conception when ovulation is restored.
Will I always need IVF if I have PCOS?
No. IVF is the last step in our protocol, recommended only when simpler approaches have not been successful, or when there is an additional fertility factor. Most PCOS patients respond well to ovulation induction with Letrozole.
Does losing weight really help with PCOS fertility?
Yes — significantly. In women with PCOS who are overweight or obese, a 5–10% reduction in body weight has been shown in multiple studies to restore spontaneous ovulation and improve pregnancy rates.
What is the risk of OHSS during IVF for PCOS patients?
PCOS patients do carry a higher risk of OHSS during IVF. At Wellspring, we manage this through personalised, low-dose stimulation protocols and a Freeze-All approach, which virtually eliminates severe OHSS.
How do PCOD/PCOS affect the success rates of other fertility treatments like IUI or IVF?
While PCOD and PCOS primarily cause fertility struggles due to irregular ovulation, they generally do not impact egg quality or ovarian reserve negatively. In fact, women with these conditions often have a robust supply of eggs. Once ovulation is successfully induced or managed through treatments like IUI Treatment or IVF, the success rates are highly favorable—frequently matching or exceeding average success rates for patients of a similar age.
What role does Metformin play if I am not diabetic but have PCOS?
Metformin is traditionally a medication used to manage type 2 diabetes, but it is highly effective for PCOS patients due to the underlying link with insulin resistance. Even if your blood sugar levels appear normal on standard tests, your body may be producing excess insulin to keep them balanced. This high level of insulin triggers the ovaries to produce excess male hormones (androgens), disrupting ovulation. Metformin helps improve your body’s insulin sensitivity, which lowers androgen production and can help restore a regular, natural menstrual cycle.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026

Begin Your PCOS Treatment Journey at Wellspring IVF, Ahmedabad
You do not need a referral. You do not need to have tried anything before. And you will leave knowing exactly where you stand and what comes next.