Diagnostic & Operative Hysteroscopy for Infertility in Ahmedabad
You have done everything right. The ovarian stimulation was excellent. The embryo was a perfect blastocyst — graded top quality by the embryologist. The transfer went smoothly. And yet — no implantation. No pregnancy.
In cases like these, the answer is often not in the embryo. It is in the room the embryo was asked to live in. The uterine cavity.
A tiny polyp acting as a physical barrier. A fine septum dividing the cavity. Invisible scar tissue from a previous procedure. A submucosal fibroid pressing on the endometrial lining. These problems are invisible on standard ultrasound. They do not appear on blood tests. But they prevent even the most genetically perfect embryo from finding its place.
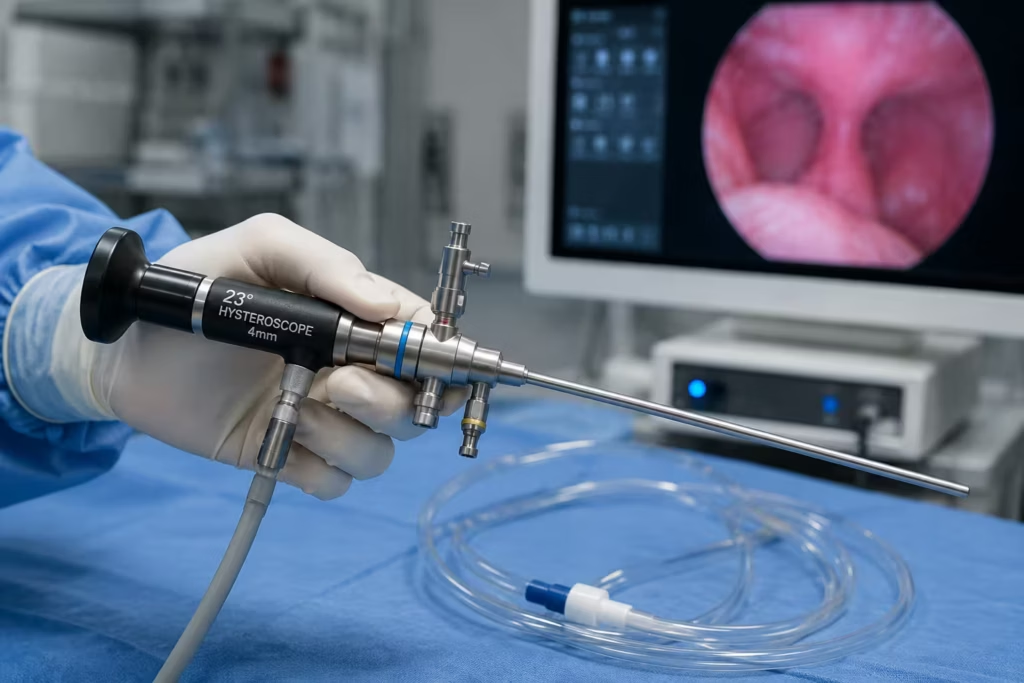
Hysteroscopy is the procedure that gives Dr. Pranay Shah a direct, magnified view of the inside of your uterus — through the natural vaginal route, without a single incision on your body. What is found is corrected in the same sitting. What was preventing implantation is removed. And the uterus is transformed into the receptive, healthy environment that a blastocyst needs.
Request a Free Callback
70%+
6,000+
3000+
15+ Yrs
Hysteroscopy vs. Laparoscopy — Understanding the Difference
One of the most frequent points of confusion among patients is the distinction between hysteroscopy and laparoscopy. Both involve a camera. Both diagnose and treat. But they examine completely different anatomical territories — and the route of access is entirely different.
The Single Most Important Distinction:
Hysteroscopy looks INSIDE the uterus — through the natural vaginal route. No body wall penetration. No incisions. No external scars.
Laparoscopy looks OUTSIDE and AROUND the uterus — through keyhole incisions in the abdomen. It examines the pelvic cavity: ovaries, fallopian tubes, and the external uterine surface.
They answer different questions. Hysteroscopy asks: ‘Is the uterine cavity structurally normal and receptive?’ Laparoscopy asks: ‘Is the pelvic environment around the uterus normal?’ Many patients need both — and Dr. Shah frequently performs both procedures on the same day under a single anaesthetic to give a complete inside + outside evaluation.
| Factor | Hysteroscopy (This Page) | Laparoscopy |
|---|---|---|
| Entry route | Through the natural vaginal and cervical canal — no body wall entry | Through small incisions in the abdominal wall |
| Cavity examined | Inside the uterus — the endometrial cavity | Outside the uterus — the pelvic cavity and abdominal organs |
| Incisions required | Zero — completely incision-free | 2–3 small keyhole incisions (5–10mm) |
| Anaesthesia | Office: local; Day care: light sedation or GA | General anaesthesia required |
| What is found | Polyps, septa, adhesions, submucosal fibroids, uterine lining quality | Endometriosis, adhesions, ovarian cysts, tubal disease, pelvic anatomy |
| Primary use | Evaluate and prepare the uterine cavity for implantation | Evaluate and treat pelvic causes of infertility |
| Typical duration | 20–45 minutes (diagnostic + minor operative) | 45–120 minutes (diagnostic + operative) |
| Hospital stay | Day care — same day discharge | Day care or one overnight stay |
| Recovery | 24–48 hours (light spotting, mild cramping) | 5–7 days (minor shoulder pain, small incision healing) |
| When combined | Often performed together on same day as laparoscopy — complete inside + outside uterine evaluation under one anaesthetic | — |
When Dr. Shah Recommends Both Together: Combined laparoscopy + hysteroscopy on the same day under one anaesthetic is recommended when the clinical picture suggests pathology both inside and outside the uterus — for example, a patient with unexplained infertility who also has a suspected polyp on ultrasound. One recovery. Complete bilateral evaluation. Often the most cost-effective and time-efficient approach for the patient.
What Happens During Hysteroscopy — Step by Step
Because hysteroscopy enters through the natural body route, many patients find the reality of the procedure far less daunting than they anticipated. Here is exactly what happens from arrival to discharge.
Preparation & Consent
You arrive fasted. Dr. Shah reviews your notes, imaging, and hysteroscopy indication. A pre-procedure consent discussion confirms what will be assessed and what is planned if pathology is found. Anaesthesia method is confirmed (local/sedation/general — see below).
Cervical Access
The hysteroscope is inserted naturally through the vagina and cervix — no incision, no cut, no stitches. For a narrow or closed cervix, a gentle dilator opens the cervical canal to 4–5mm. For postmenopausal patients or nulliparous women, this step may take slightly longer.
Uterine Distension with Fluid
Sterile saline or CO₂ gas is gently instilled through the hysteroscope to expand the uterine cavity — creating a clear viewing space between the uterine walls. This is what ‘opens’ the cavity to allow complete 360° inspection.
Systematic Cavity Survey - Diagnostic Phase
Dr. Shah performs a complete, methodical inspection: the cervical canal, the internal os, the uterine fundus, both tubal ostia (openings of the fallopian tubes), the anterior wall, posterior wall, and both lateral walls. Everything is visible in high-definition on the operating monitor. The endometrial lining quality, any polyps, fibroids, adhesions, or septal tissue are directly visualised.
Operative Treatment - Same Sitting
If pathology is identified, specialised miniature instruments (scissors, resectoscope loop, bipolar forceps, mechanical morcellator) are introduced through the operative channel of the hysteroscope. Polyps are excised. Septa are incised. Adhesions are divided. Submucosal fibroids are resected. The procedure is performed under direct vision — Dr. Shah sees every movement of every instrument relative to the uterine walls in real time.
Fluid Balance Monitoring
During operative hysteroscopy, the nursing team continuously monitors fluid input and output — tracking the balance between distension fluid used and recovered. Excess fluid absorption is a safety parameter that guides the safe duration of the operative phase.
Withdrawal & Recovery
The hysteroscope is gently withdrawn. No sutures required — no skin closure needed. You are moved to the recovery area. Light bleeding and mild cramping are normal for 24–48 hours post-procedure.
| Anaesthesia Type | When Used | Patient Experience |
|---|---|---|
| Local anaesthesia (paracervical block) | Diagnostic hysteroscopy only, cooperative patient, thin cervix | Awake throughout. Mild cramping sensation — similar to period pain. No sedation recovery time. Same-day return to work possible. |
| Conscious sedation (IV sedation) | Diagnostic + minor operative. Anxious patients. Moderate procedures. | Drowsy but semi-conscious. No pain experienced. Short recovery 1–2 hours. Day-care discharge. |
| General anaesthesia (GA) | Complex operative procedures — septum resection, severe Asherman’s, large fibroid resection, combined lap + hystero | Fully asleep. Complete pain-free procedure. Recovery 2–4 hours post-procedure. Same-day or one night. |
Dr. Pranay Shah on Hysteroscopy: “When I explain to a patient that I will be looking inside the uterus without making a single cut on the outside of the body, there is always a moment of visible relief. The camera enters through the same route as a routine gynaecological examination. For a diagnostic procedure, many of my patients describe it as less uncomfortable than they expected. The technology has improved so dramatically in the last decade that what once required a full hospital admission is now routinely done as a day-care procedure — and in some cases, even in the office.”
The Uterine Cavity and Implantation — Why the “Room” Matters
Embryo implantation is a molecular conversation between the blastocyst and the endometrial lining — a tightly timed dialogue of adhesion molecules, cytokines, and receptivity signals. But this conversation cannot happen if the physical structure of the room is compromised.
What a Receptive Uterine Cavity Looks Like
- Smooth, uniform endometrial lining — 8–12mm triple-line pattern on scan
- No intrusions — no polyps, no fibroids projecting into the space
- No physical divisions — no septum splitting the cavity
- No adhesions — walls move freely, cavity opens symmetrically
- Both tubal ostia visible and clear at the fundus
- Uniform, healthy pink vascularity throughout — no pale, scarred patches
This is the uterus that welcomes and sustains an embryo.
What Prevents Implantation in a Compromised Cavity:
- Polyp: acts as a physical ‘IUD’ — blocks embryo from attaching at the polyp site; alters local prostaglandin environment unfavourably
- Submucosal fibroid: displaces endometrium, reduces blood flow, creates mechanical distortion
- Septum: poorly vascularised fibrous tissue — embryo implants but cannot develop; miscarriage follows
- Adhesions (Asherman’s): large areas of cavity fused together — no space, no lining, no implantation
- Endometritis (subclinical): inflamed lining that fails to express implantation receptivity signals
Even the best IVF embryo cannot overcome a structurally hostile cavity.
What the Evidence Says About Uterine Cavity Abnormalities Before IVF:
Multiple published studies have assessed the prevalence of uterine cavity abnormalities in women presenting for IVF — women who were not suspected of having any uterine problem:
- A 2019 TROPHY trial found that hysteroscopy in women with recurrent implantation failure (≥3 failed IVF cycles) did NOT improve outcomes — important for patient counselling (hysteroscopy is not a blanket pre-IVF treatment)
- However, in women with a suspected uterine cavity abnormality on ultrasound or sonohysterography, correcting it before IVF improves live birth rates by 15–40% depending on the specific pathology
- Endometrial polyps: removal before IVF increases clinical pregnancy rates (meta-analysis: OR 2.1, i.e. doubled odds of clinical pregnancy)
- Uterine septum: associated with 60–65% miscarriage rate when untreated; after septum resection, miscarriage risk reduces to near-population levels
- Asherman’s syndrome: live birth rate with moderate-to-severe adhesions before treatment is very low; after successful adhesiolysis, a viable pregnancy becomes achievable
Dr. Shah’s principle: hysteroscopy is not recommended for every IVF patient as a routine step — it is indicated when there is a clinical reason to suspect or evaluate the uterine cavity.
Conditions Diagnosed and Treated by Dr. Pranay Shah at Hysteroscopy
Endometrial Polyps — Hysteroscopic Polypectomy
Smooth, soft overgrowths of the uterine lining — the single most common structural cause of unexplained infertility and failed IVF
What Dr. Shah Sees on the Monitor:
An endometrial polyp is a localised overgrowth of endometrial tissue — a finger-like or rounded projection extending from the uterine wall into the cavity. Polyps appear as smooth, vascular, mobile structures — pale pink to deep red, with a visible stalk (pedunculated) or a broad base (sessile). On standard 2D ultrasound, small polyps are easily missed — they blend with the endometrial lining. Saline infusion sonography (SIS/sonohysterography) improves detection, but hysteroscopy remains the gold standard both for definitive diagnosis and for removing the polyp under direct vision.
How It Is Treated in the Same Sitting:
- Hysteroscopic polypectomy: the polyp is grasped with forceps and the stalk is cut with miniature scissors or an electrocautery loop — the entire polyp, including its base, is removed
- Complete removal confirmed: Dr. Shah directly inspects the site of excision — no residual polyp tissue is left behind
- The polyp is sent for histological examination (tissue analysis) as routine — to confirm the benign nature and rule out any atypical endometrial cells
- Recovery: light spotting for 2–5 days. Next period typically arrives on schedule. IVF or natural conception attempts can begin from the following menstrual cycle.
Clinical Evidence:
Removal of endometrial polyp before IVF: clinical pregnancy rate improvement documented across multiple RCTs (meta-analysis odds ratio approximately 2.1 — doubling of clinical pregnancy rates compared to leaving the polyp in place).
→ Read more: Uterine Polyps — Complete Guide
Submucosal Fibroids — Hysteroscopic Myomectomy
Fibroids that project into the uterine cavity — the most fertility-impairing fibroid type
What Dr. Shah Sees on the Monitor:
Submucosal fibroids (Type 0, Type 1, and Type 2 in the FIGO classification system) are the most clinically significant fibroids for fertility — they project into the endometrial cavity itself, directly disrupting the implantation surface. On hysteroscopy, they appear as hard, pale, firm rounded masses distorting the cavity — unlike the soft, mobile polyp, the fibroid resists compression and has a paler, less vascular surface. The degree of intracavity protrusion determines whether hysteroscopic removal is feasible (Type 0: fully intracavitary — ideal; Type 1: >50% intracavitary; Type 2: <50% intracavitary — may require combination approach).
How It Is Treated in the Same Sitting:
- Hysteroscopic myomectomy using a resectoscope: a fine wire loop attached to an electrosurgical generator slices through the fibroid tissue under direct vision
- The fibroid is progressively shaved and resected until the cavity is fully restored to a smooth, unobstructed state
- Type 0 and Type 1 fibroids: typically completed in a single hysteroscopy session
- Type 2 and larger fibroids: may require staged hysteroscopy (two sessions 4–6 weeks apart) to complete the resection safely and allow the myometrium to regenerate
- Advantage over open myomectomy: no abdominal incision, no uterine scar, lower adhesion risk, faster return to fertility attempts
→ Read more: Uterine Fibroids — Detailed Guide
Uterine Septum — Hysteroscopic Septum Resection (Metroplasty)
The most common congenital uterine anomaly — and the most significant correctable cause of recurrent miscarriage
What Dr. Shah Sees on the Monitor:
A uterine septum is a fibrous tissue wall that hangs down from the fundus (top) of the uterine cavity, dividing it partially (incomplete septum — 70% of cases) or completely (complete septum, extending to the cervix — 30% of cases). It forms during foetal development when the two Mullerian ducts fail to reabsorb their shared wall completely. The septum is composed predominantly of fibrous connective tissue with poor blood supply — a placenta or embryo that implants on the septum cannot develop adequately. The result: recurrent first-trimester miscarriage.
How It Is Treated in the Same Sitting:
- Hysteroscopic septum resection (metroplasty): using microscissors or a fine electrosurgical needle, the septum is divided from its free edge progressively towards the fundus — until the cavity is reunified into a single, triangular, normally shaped space
- Laparoscopic guidance simultaneously: a laparoscope is frequently used at the same time to watch the outer uterine surface — preventing inadvertent fundal perforation as the septum is divided from inside
- No uterine scar created: unlike open metroplasty, the hysteroscopic approach creates no incision in the uterine wall — preserving full structural integrity for pregnancy
- Post-procedure hormonal support: oestrogen therapy is often prescribed for 4–6 weeks post-resection to promote healthy endometrial regrowth across the resected septum base
Clinical Evidence:
Uterine septum is associated with a miscarriage rate of 60–65% and a live birth rate of only 25–35% when untreated. After successful hysteroscopic septum resection, miscarriage rate falls to 10–15% (near population baseline) and live birth rate rises to 75–80%.
→ Read more: Recurrent Miscarriage — Complete Guide
Asherman's Syndrome — Hysteroscopic Adhesiolysis
Intrauterine scar tissue — most commonly from prior D&C, post-partum curettage, or uterine infection
What Dr. Shah Sees on the Monitor:
Asherman’s syndrome (intrauterine adhesions, IUA) describes the formation of scar tissue bands within the uterine cavity — thin fibrous bridges between opposite walls, or dense, vascular adhesions obliterating large sections of the cavity. The endometrial lining is replaced by scar tissue that cannot respond to hormonal stimulation or support implantation. Clinical signs include: reduced or absent menstruation after a uterine procedure (D&C, evacuation of retained products, postpartum curettage), cyclical pelvic pain with no visible bleed, and infertility or recurrent miscarriage. On hysteroscopy, adhesions appear as pale, avascular bands stretched across the cavity — the classic appearance is a cavity that looks partitioned or bridged.
How It Is Treated in the Same Sitting:
- Hysteroscopic adhesiolysis: adhesion bands are carefully divided with miniature scissors or a fine electrosurgical needle — always under direct vision
- Severity determines approach: mild/moderate adhesions (AFS Grade I–II) are divided in a single session. Severe adhesions (Grade III) may require staged hysteroscopy with intrauterine balloon placement between sessions to prevent re-adhesion
- Post-procedure: intrauterine balloon or Foley catheter may be placed for 5–7 days to keep cavity walls separated during initial healing
- High-dose oestrogen support for 6–8 weeks post-procedure to stimulate regeneration of the endometrial lining over the healed adhesion sites
- Follow-up hysteroscopy: a second hysteroscopy is performed 6–8 weeks later to confirm cavity restoration and identify any re-adhesion that requires further treatment
- Prognosis: depends critically on severity — mild Asherman’s responds well, with near-normal reproductive outcomes. Severe obliterative Asherman’s has a more guarded prognosis and may require multiple procedures.
→ Read more: Recurrent Miscarriage — Uterine Causes
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
When Dr. Pranay Shah Recommends Hysteroscopy — and When He Does Not
Hysteroscopy IS Recommended When:
- Endometrial polyp confirmed or suspected on transvaginal ultrasound, SIS, or sonohysterography
- Submucosal fibroid identified on scan — intracavitary or significant bulge into the cavity
- Uterine septum diagnosed on 3D ultrasound or MRI
- Recurrent miscarriage (2+ losses) — uterine structural cause investigation
- Two or more failed IVF cycles with good-quality embryos — ruling out missed cavity abnormality
- Reduced or absent periods after a uterine procedure (D&C, delivery) — suspected Asherman’s
- Abnormal uterine bleeding requiring cavity evaluation
- Before first IVF cycle when there is a specific clinical finding on scan — not as routine universal screening
- Combined with laparoscopy when both inside and outside uterus need evaluation together
Hysteroscopy Is NOT Recommended When:
- Normal uterine cavity on multiple concordant scans with no symptoms suggesting a cavity problem — routine pre-IVF hysteroscopy in this group is not evidence-based (see TROPHY trial 2019)
- Active pelvic or uterine infection — procedure risk is higher during active infection; infection must be treated first
- Confirmed intrauterine pregnancy — hysteroscopy is contraindicated
- Heavy active uterine bleeding — reduces visibility, increases risk
- When male factor infertility is the sole identified cause — uterine surgery does not address a sperm problem
Dr. Shah on selective hysteroscopy: ‘The TROPHY trial was important — it reminded us that performing hysteroscopy on every patient before IVF, without a specific reason, does not improve IVF outcomes. I recommend hysteroscopy when I have a clinical reason. Not as a ‘let us check just in case’ procedure to add cost to a cycle.’
What Our Patients Say
[sseo-reviews-list category=’4′ type=’Slider’ limit=’4′ textlimit=’250′]
Join 500+ Satisfied Families
Hysteroscopy Before IVF — The Strategic Decision
The question “Should I have a hysteroscopy before starting IVF?” is one of the most frequently discussed decisions in Dr. Shah’s pre-IVF consultation. The answer depends entirely on what your investigations show.
| Clinical Situation | Hysteroscopy Before IVF? | Rationale | What Happens After |
|---|---|---|---|
| Endometrial polyp on ultrasound or SIS | YES — recommended | Polyp doubles IVF failure risk. Removal improves pregnancy rates significantly. | IVF can begin from the next cycle after polypectomy. |
| Submucosal fibroid (Type 0 or Type 1) | YES — strongly recommended | Intracavitary fibroid directly obstructs implantation space and disrupts vascularity. | IVF begins 1–2 cycles after fibroid resection and cavity healing. |
| Uterine septum diagnosed on 3D scan or MRI | YES — before IVF or conception attempts | Without resection, miscarriage risk remains very high even if IVF succeeds initially. | IVF or natural attempts begin 2–3 months after resection and hormonal support. |
| 2+ failed IVF cycles, good embryos, no known cause | YES — investigation recommended | 15–35% have an undiagnosed cavity problem. | Further IVF cycle begins after cavity pathology is corrected. |
| Suspected Asherman’s — reduced periods post-D&C | YES — diagnostic + therapeutic | Adhesions can prevent implantation entirely. | Further cycles after confirmed cavity restoration on follow-up hysteroscopy. |
| Normal cavity on multiple concordant scans, first IVF attempt | NOT routinely recommended | No evidence that routine pre-IVF hysteroscopy improves outcomes in normal cavities. | Proceed directly to IVF stimulation. Hysteroscopy if first cycle fails. |
| Normal cavity, second IVF attempt, first transfer failed | Consider — case-by-case | After one failed transfer with a good embryo, cavity review becomes appropriate. | If scan remains normal, proceed. If any finding, treat first. |
➡️ After Hysteroscopy — The Pathway to Implantation at Wellspring
Surgery prepares the ground. What follows depends on the full clinical picture:
- Frozen Embryo Transfer (FET) — if embryos are already banked from a previous stimulation cycle, FET can begin from the next cycle after cavity restoration. FET into a perfectly prepared cavity is the optimal post-hysteroscopy pathway.
- Fresh IVF Cycle — for patients starting IVF after hysteroscopy for the first time. Stimulation begins once the cavity has fully healed.
- Natural conception — for patients with patent tubes and good ovarian reserve, particularly after polypectomy or mild adhesiolysis: spontaneous conception in the window after hysteroscopy is well-documented.
- Recurrent Miscarriage investigation — for septum and Asherman’s patients, a complete recurrent miscarriage workup (clotting profile, immunological factors, chromosomal analysis of couple and products of conception) may be recommended alongside hysteroscopy
Talk to Dr. Shah About Cavity Optimisation
Recovery After Hysteroscopy — What to Expect
| Timeframe | What You Experience | Activity Level |
|---|---|---|
| During procedure | Under local, sedation, or GA — no pain experienced during the procedure itself. | — |
| 0–4 hours post-procedure | Waking from anaesthesia if sedation/GA used. Mild cramping. Light vaginal spotting begins. | Resting in recovery. Same-day discharge for most patients. |
| Day 1–2 | Mild-moderate cramping, especially for operative cases. Light spotting or bleeding. Mild bloating from distension fluid. | Rest at home. No heavy lifting. Light household activity is fine. |
| Day 3–5 | Cramping resolves. Spotting reduces to very light. Most patients feel normal. | Return to desk work. Normal activity except swimming or tampon use until spotting stops. |
| Day 5–7 | Full return to normal activity for the majority of patients. | Normal including gentle exercise. |
| Next menstrual cycle | First period arrives approximately on schedule. The endometrium regenerates fully within one cycle. | Fertility attempts can begin from this cycle for polypectomy and minor cases. |
| Post-septum / Asherman’s | Hormonal support for 4–8 weeks. Follow-up hysteroscopy at 6–8 weeks to confirm cavity restoration. | Fertility attempts begin after confirmed cavity restoration. |
-Fever above 38°C (100.4°F) at any point post-procedure
-Heavy vaginal bleeding — soaking more than one pad per hour for 2+ hours
-Severe abdominal pain that is worsening rather than improving
-Foul-smelling vaginal discharge suggesting infection
-No menstrual period within 8 weeks of hysteroscopy — particularly after Asherman's treatment
 Wellspring IVF post-procedure helpline: 9099946050
Wellspring IVF post-procedure helpline: 9099946050Frequently Asked Questions
Is hysteroscopy painful?
The experience depends on the anaesthesia used. A diagnostic hysteroscopy under local anaesthesia produces mild cramping — described by most patients as similar to a period cramp. Under conscious sedation, no pain is experienced at all during the procedure — only mild discomfort on waking. Under general anaesthesia (for operative cases), there is complete insensibility throughout. After the procedure, mild-moderate cramping for 24–48 hours is normal for operative cases. Over-the-counter analgesics (ibuprofen or paracetamol) manage this effectively for the large majority of patients.
Does hysteroscopy leave any scars?
No — this is one of hysteroscopy’s most significant advantages. Because the hysteroscope enters through the natural vaginal route, there is absolutely no external incision, no abdominal scar, and no stitches. Even internally, the operative procedures (polypectomy, septum resection, adhesiolysis) are designed to create the minimal amount of internal trauma — the goal is restoration of normal tissue architecture, not addition of new wound surfaces.
How soon after hysteroscopy can I attempt IVF or natural conception?
For endometrial polypectomy and minor operative hysteroscopy: from the very next menstrual cycle — typically 4–6 weeks after the procedure. For uterine septum resection: after 6–8 weeks of hormonal support and a confirmatory follow-up hysteroscopy showing healed cavity — typically 2–3 months. For Asherman’s adhesiolysis: after confirmed cavity restoration on follow-up hysteroscopy and full endometrial regeneration — typically 3–4 months for moderate cases, potentially longer for severe Asherman’s.
I've had two failed IVF cycles. Will hysteroscopy help?
It may — this is exactly the indication that has the strongest clinical justification for hysteroscopy. In women with recurrent implantation failure (good embryos, no implantation), studies consistently show that 15–35% have a previously undiagnosed uterine cavity abnormality. A diagnostic hysteroscopy in this group identifies and corrects these lesions — and subsequent IVF cycles show significantly improved implantation rates. Dr. Shah would also recommend a comprehensive recurrent implantation failure workup (endometrial receptivity assessment, thrombophilia screen, immunological evaluation, and PGT-A on embryos) alongside hysteroscopy — since multiple factors often contribute.
What is the difference between a hysteroscopy and a D&C?
A D&C (dilation and curettage) is a blind procedure — the cervix is dilated and a curette is swept inside the uterus without any direct visual guidance. The surgeon cannot see what they are removing or where they are in the cavity. Hysteroscopy is the precise opposite — a camera provides direct, magnified, real-time visualisation of every structure inside the uterus before any instrument is used. Hysteroscopy identifies and removes specific lesions (polyps, fibroids, septa, adhesions) with surgical precision. D&C is non-selective and is a known cause of Asherman’s syndrome when performed repeatedly. For fertility purposes, hysteroscopy is always the preferred, evidence-based approach over blind D&C.
I've been told I have a uterine septum. Will I need surgery before trying naturally?
A uterine septum significantly increases miscarriage risk — published data consistently show a 60–65% miscarriage rate in women with an untreated septum versus 10–15% after hysteroscopic resection. Dr. Shah typically recommends septum resection before fertility treatment (whether natural conception, IUI, or IVF) for this reason: it is a relatively straightforward hysteroscopic procedure with a very favourable risk-benefit profile, and it converts a very high-risk uterine environment into a near-normal one. The procedure takes 30–45 minutes, recovery is 2–3 months, and the subsequent improvement in pregnancy outcome is substantial. Read more: Recurrent Miscarriage Guide
What is the cost of hysteroscopy in Ahmedabad?
The cost depends on the type of procedure — a diagnostic hysteroscopy with minor polypectomy is priced differently from a complex operative case such as septum resection or severe Asherman’s adhesiolysis. At Wellspring, Dr. Shah provides a complete itemised cost estimate during your pre-operative consultation, based on the findings expected and the procedure planned. There are no hidden charges for findings addressed during the same sitting. For current pricing, call 9099946050.
Related Conditions & Treatments
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
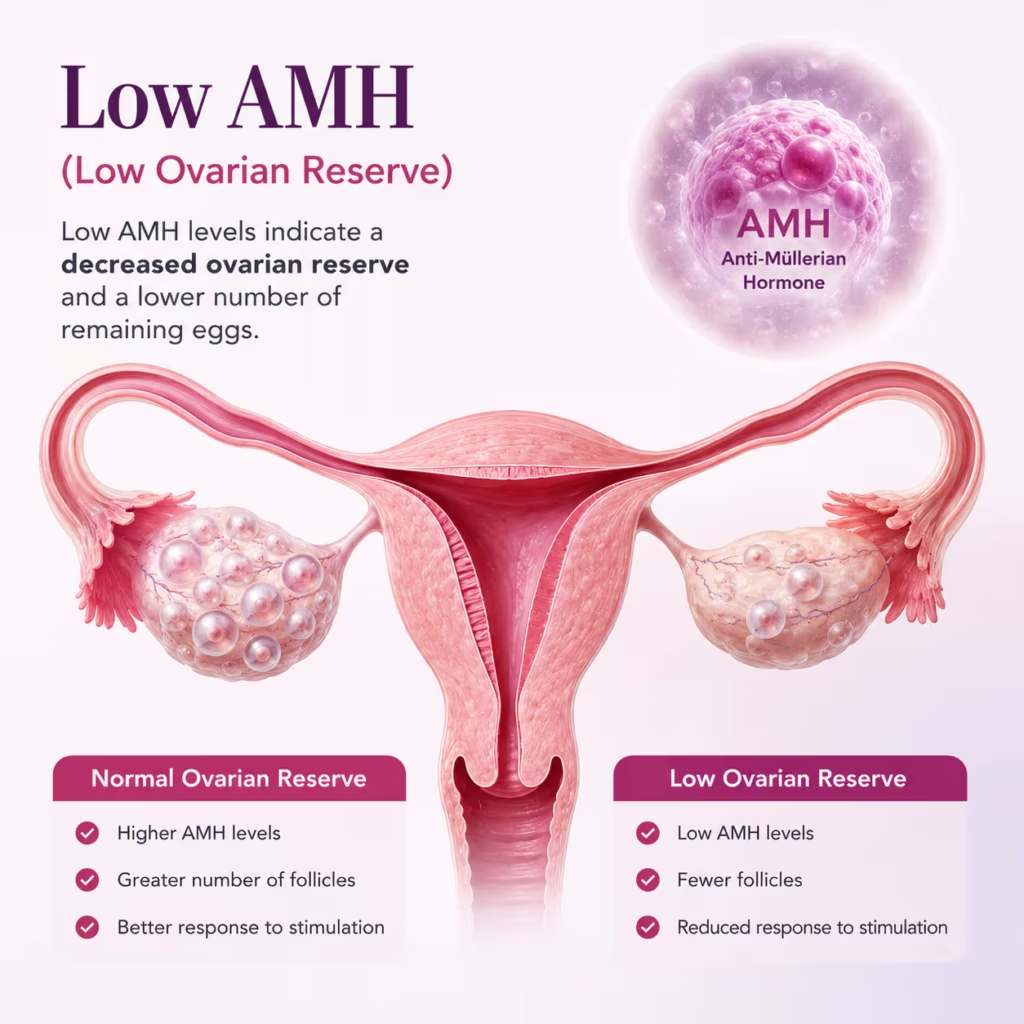
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026