Uterine Fibroids Treatment in Ahmedabad— Location Matters More Than Size
The vast majority of uterine fibroids do not require surgery.
Fibroids are non-cancerous muscular growths. They are extraordinarily common — present in up to 40% of women of reproductive age. In most of these women, the fibroids cause no symptoms, pose no threat to fertility, and require nothing more than a watchful eye on follow-up scanning.
The question is never simply: "Do I have fibroids?" The question that actually determines your treatment path is: "Where are my fibroids located, and are they affecting my uterine cavity?"
At Wellspring IVF & Women's Hospital, Dr. Pranay Shah is known for an approach that runs counter to the reflex to operate: he evaluates each fibroid on its own clinical merits. When surgery is needed, he performs uterus-sparing laparoscopic myomectomy — preserving the uterus and protecting future fertility. When surgery is not needed, he says so — clearly, honestly, and with evidence.
The Most Important Sentence on This Page
A 1cm submucosal fibroid sitting inside the uterine cavity causes significantly more damage to fertility and implantation than a 6cm subserosal fibroid sitting quietly on the outside of the uterus.
Location determines clinical significance. Size alone is not a reason for surgery.
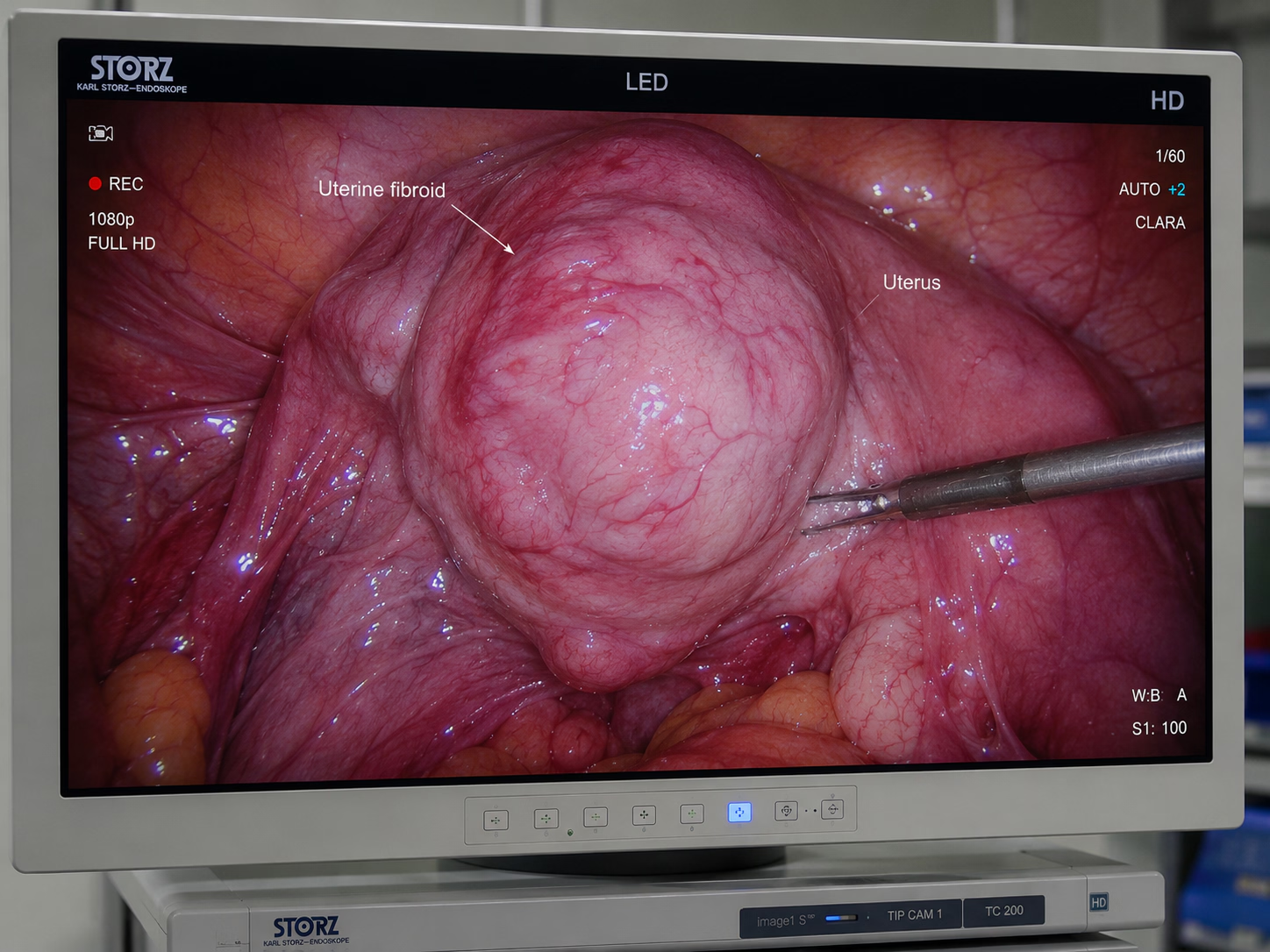
What Are Uterine Fibroids?
Uterine fibroids — also called myomas or leiomyomas — are benign (non-cancerous) tumours made of smooth muscle tissue that grow in or around the uterus. They are not cancer. They cannot become cancer. And in the majority of women, they never cause any significant problem.
Their growth is driven primarily by oestrogen and progesterone — which is why they tend to develop during the reproductive years and typically shrink or stabilise after menopause. They vary enormously in size — from a few millimetres to, in rare cases, several centimetres.
The reason fibroids matter in the context of fertility is anatomical, not oncological. When a fibroid grows in a location that physically distorts the uterine cavity — the space where an embryo must implant — it interferes mechanically with implantation. When it does not touch the cavity, the uterus functions normally and fertility is unaffected.
Watch Our Fibroid Treatment Video
Learn how uterine fibroids affect fertility and when treatment may be needed before pregnancy or IVF.
What You Will Learn
Understand how fibroid size and location can influence fertility and treatment decisions.
- Fibroids and fertility explained
- When fibroid surgery is needed
- Fibroid location and pregnancy impact
- Treatment options before IVF
The 4 Types of Uterine Fibroids — Location Is Everything
Understanding which type of fibroid you have is the single most important step in deciding whether treatment is needed. Here is the complete classification
| Type | Location | Fertility & Pregnancy Impact | Surgery Needed? |
|---|---|---|---|
| Submucosal (Type 0, 1, 2) | Inside or bulging into the uterine cavity | HIGHEST impact. Directly blocks embryo implantation. Associated with recurrent miscarriage and IVF failure | YES — Hysteroscopic resection (Type 0/1) or Myomectomy (Type 2) |
| Intramural (Type 3–5) | Within the muscular wall of the uterus | Moderate impact IF large (>4–5cm) and distorting cavity. Smaller intramural fibroids may not affect fertility | Depends on size & cavity distortion. MRI helps assess |
| Subserosal (Type 6–7) | On the outer surface of the uterus, projecting outward | LOWEST impact on fertility. Rarely affects the uterine cavity. May cause pelvic pressure/bulk symptoms | Rarely for fertility. Only if causing pressure symptoms |
| Pedunculated | Stalked fibroid hanging off outer uterus or within cavity | Submucosal pedunculated: high impact. Subserosal pedunculated: low fertility impact | If submucosal: YES. If subserosal: only for symptoms |
FIGO Classification Note
The FIGO (International Federation of Gynaecology and Obstetrics) classification system grades fibroids 0–8 based on position relative to the uterine cavity. Type 0 = fully inside the cavity. Type 8 = far outside the uterus (e.g., cervical). Dr. Shah uses this classification to guide surgical decisions. When relevant, he requests an MRI pelvis for accurate grading prior to planning surgery.
Size vs. Location — The Truth About Fibroids and Fertility
One of the most common mistakes in fibroid management is treating size as the primary decision-making variable. It is not. Here is how the two factors compare in clinical importance:
| Size Alone (Misleading) | Location (What Actually Matters) |
|---|---|
| “6cm fibroid — needs surgery” | A 6cm subserosal fibroid outside the uterus may have zero impact on fertility |
| “3cm fibroid — wait and watch” | A 3cm submucosal fibroid inside the cavity must be removed before IVF or conception |
| “Multiple fibroids — high risk” | Multiple subserosal fibroids with an undistorted cavity may not require surgery at all |
| “Large fibroid before IVF — remove it” | Removal decision depends on whether the fibroid distorts the cavity — not on size alone |
| “Small fibroid — no concern” | A small submucosal fibroid (even <2cm) is a direct barrier to embryo implantation |
How Dr. Shah Evaluates Your Fibroid
- Transvaginal Ultrasound (TVS): First assessment of number, size, and position of fibroids. Identifies any submucosal component.
- Saline Infusion Sonography (SIS) / Sonohysterography: Saline injected into the uterine cavity under ultrasound. Precisely maps the relationship of the fibroid to the uterine cavity — more accurate than standard ultrasound for submucosal assessment.
- MRI Pelvis: Requested for large fibroids, multiple fibroids, or cases where surgery is being planned. Provides exact FIGO grade, depth of myometrial penetration, and proximity to important structures.
- Hysteroscopy: Direct visual inspection of the uterine cavity. Definitive for identifying submucosal fibroids. Allows simultaneous treatment of Type 0 and Type 1 fibroids in the same procedure.
Fibroids and Fertility — When Do They Actually Cause Problems?
The evidence-based answer, summarised: submucosal fibroids reduce IVF success rates by approximately 30–50% and must be removed before embryo transfer. For other types, the evidence is more nuanced
Submucosal Fibroids — Remove Before IVF or Pregnancy Attempt
Mechanism: In cases of a submucosal fibroid IVF success can be severely hindered because these growths alter the uterine environment in multiple ways: they distort the cavity geometry, impair endometrial blood flow, trigger a local inflammatory response, and physically occupy the space where an embryo must attach.
The evidence: A Cochrane review and multiple meta-analyses confirm that submucosal fibroids reduce implantation rates, clinical pregnancy rates, and live birth rates by 30–50% in IVF cycles. Removal restores these rates to baseline.
Recommendation: Remove all submucosal fibroids (FIGO Type 0, 1, and Type 2 where cavity is distorted) before attempting IVF or natural conception if recurrent failure has occurred.
Surgical method: Type 0 and Type 1: Hysteroscopic resection (no incision, through cervix, day procedure). Type 2 and larger: Laparoscopic myomectomy.
Large Intramural Fibroids — Evaluate Individually
The threshold: Intramural fibroids larger than 4–5 cm that distort the uterine cavity are associated with reduced IVF success rates. Those that do not reach or distort the cavity may not require removal before fertility treatment.
The investigation: MRI pelvis is essential for intramural fibroids being considered for surgery. It maps the exact position of the fibroid relative to the endometrium (uterine lining) and the serosa (outer surface).
Surgical consideration: Laparoscopic myomectomy for fibroids distorting the cavity. A 3–6 month healing period is recommended before IVF — the uterine scar must fully heal before embryo transfer or pregnancy.
The risk of over-treatment: Removing large intramural fibroids carries a small risk of uterine rupture in pregnancy if the myometrium was deeply penetrated. This risk must be weighed against the fertility benefit. Dr. Shah discusses this openly.
Subserosal & Pedunculated Fibroids — Usually Watch and Wait
The evidence: Subserosal fibroids — those growing outward from the uterine surface — do not alter the uterine cavity and are generally not associated with reduced fertility or IVF failure rates.
When Dr. Shah recommends surgery: Subserosal fibroids causing significant pelvic pressure, bladder compression, or pain that impairs quality of life. Not for fertility reasons unless very large (>8–10cm) and causing anatomical distortion.
Pedunculated subserosal fibroids: Stalked fibroids hanging off the outer uterus. Rarely affect fertility. May occasionally tort (twist on their stalk), causing acute pain. Surgical removal only if symptomatic.
The right advice: A woman with multiple subserosal fibroids and a clean uterine cavity can proceed to IVF without any fibroid surgery. Doing unnecessary surgery before IVF wastes time and creates recovery delays.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Symptoms of Uterine Fibroids — What to Watch For
Many fibroids are entirely asymptomatic — discovered incidentally on a routine scan. When symptoms do occur, they typically include
Symptomatic Fibroids | Silent Fibroids (Common) |
|---|---|
Heavy, prolonged periods (menorrhagia) | No periods symptoms at all |
Pelvic pressure, bloating, heaviness | Discovered on routine scan only |
Frequent urination (bladder compression) | Normal fertility — subserosal only |
Recurrent miscarriage or IVF failure | No pain, no bleeding abnormality |
Anaemia from chronic blood loss | Asymptomatic across reproductive years |
Pain during periods or intercourse | Shrink naturally after menopause |
Ready To Begin Your Fertility Journey?
Laparoscopic Myomectomy — Uterus-Sparing Surgery by Dr. Pranay Shah
When fibroid surgery is clinically indicated, Dr. Pranay Shah performs laparoscopic (keyhole) myomectomy — a minimally invasive procedure that removes the fibroid while preserving the uterus completely. This is the most important distinction: myomectomy removes the fibroid. The uterus remains intact.
Laparoscopic Myomectomy — What to Expect
Approach
3–4 small keyhole incisions (5–10mm each) in the abdomen. A laparoscope (camera) and instruments are inserted. The fibroid is identified, dissected from the uterine wall, and removed. The uterine defect is sutured in multiple layers to restore uterine integrity.
Anaesthesia
General anaesthesia. Procedure time: 1–3 hours depending on fibroid size and number.
Hospital stay
Typically 1–2 days. Most women return to normal activity within 2 weeks.
Recovery before IVF/Pregnancy
Dr. Shah recommends a 3–6 month healing period after myomectomy before attempting IVF or natural conception. This allows the uterine scar to fully heal and mature — reducing the small risk of uterine rupture during pregnancy.
Advantage over open surgery
Significantly less blood loss, faster recovery, less adhesion formation (scar tissue), and better cosmetic outcome than open (abdominal) myomectomy.
Advantage over hysterectomy
The uterus is completely preserved. Fertility is maintained. This is not a consideration for women who have completed their families, but it is critical for women still planning pregnancy.
Recurrence
Fibroids can recur after myomectomy — particularly if multiple fibroids were present. The recurrence rate is approximately 10–15% at 5 years. Dr. Shah discusses this as part of pre-surgical counselling.
Hysteroscopic Myomectomy — For Submucosal Fibroids (Type 0 & 1)
- What it is: A hysteroscope (thin camera) is passed through the cervix — no incisions, no external cuts. The submucosal fibroid is visualised inside the uterine cavity and resected (shaved down) using an electrosurgical loop.
- Best for: FIGO Type 0 (fully inside cavity) and Type 1 (majority inside cavity). Some Type 2 fibroids can also be treated hysteroscopically in experienced hands.
- Anaesthesia: General anaesthesia or sedation. Day procedure — home same day.
- Recovery:1–2 weeks before fertility treatment can resume. This is the fastest timeline to clear a submucosal fibroid IVF barrier and return safely to embryo transfer protocols.
- Read more: Hysteroscopy at Wellspring IVF — full procedure guide on our Hysteroscopy page.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Fibroids vs. Adenomyosis — Two Different Conditions, Often Confused
Fibroids and Adenomyosis are frequently confused — both affect the uterus, both cause heavy periods, and both impact fertility. However, they are fundamentally different conditions requiring different treatment approaches:
| Uterine Fibroids | Adenomyosis | |
|---|---|---|
| What it is | Distinct muscular growth (tumour) | Endometrial tissue within muscle wall |
| Appearance on scan | Distinct round mass on ultrasound | Bulky, globular uterus; asymmetric wall |
| Diagnosis | Ultrasound or MRI | Ultrasound, MRI, or laparoscopy |
| Can it be removed? | Yes — myomectomy | No — diffuse disease, not a discrete mass |
| Symptoms | Often silent. Heavy periods, bulk | Painful periods, heavy bleeding, deep pain |
| Fertility impact | Only if submucosal/cavity distortion | Impairs implantation, IVF success rates |
| Treatment options | Myomectomy / Hysteroscopic resection | GnRH therapy, IVF, in severe cases hysterectomy |
If you have a bulky, globular uterus with heavy painful periods and you have been told you have fibroids — ask whether adenomyosis has been specifically excluded. The two conditions frequently coexist, and missing adenomyosis changes the treatment plan significantly. Read our full guide: Adenomyosis Treatment at Wellspring IVF.
Related Conditions & Treatments at Wellspring IVF
“I meet women who have been scheduled for myomectomy for a 4cm subserosal fibroid that is sitting quietly on the outside of their uterus, causing zero interference with the cavity. And I meet women with a 1.5cm submucosal fibroid that has been on the “watch and wait” list for two years — while they have had three failed IVF cycles. The fibroid that is inside the cavity always needs to be dealt with first. The fibroid outside never did.”
— Dr. Pranay Shah, MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
Frequently Asked Questions
I have fibroids. Do I need surgery before trying to get pregnant?
Not necessarily — and possibly not at all. The decision depends entirely on the location of your fibroid. If your fibroid is submucosal (inside or protruding into the uterine cavity), it should be removed before any attempt at natural conception or IVF — the evidence is clear that it reduces success rates. If your fibroid is subserosal (outside the uterus) and your cavity is unaffected, surgery is very likely unnecessary before fertility treatment. Dr. Shah will evaluate your specific fibroid with an ultrasound and, if needed, an MRI.
Can I do IVF with fibroids?
Yes — if the fibroid is subserosal and not distorting the uterine cavity, IVF can proceed without fibroid surgery. If the fibroid is submucosal or if it is a large intramural fibroid distorting the cavity, it should be removed first. At Wellspring IVF, Dr. Shah evaluates the uterine cavity precisely before every IVF cycle using saline sonography or hysteroscopy to confirm the cavity is clear before proceeding.
What is a laparoscopic myomectomy and how is it different from a hysterectomy?
A myomectomy removes only the fibroid — the uterus is completely preserved. A hysterectomy removes the entire uterus. For any woman who still wants to conceive, hysterectomy is never the appropriate choice for fibroid treatment. Dr. Pranay Shah performs uterus-sparing laparoscopic myomectomy — a keyhole procedure that removes the fibroid through small incisions while leaving the uterus intact and fully functional.
How long after myomectomy can I try IVF or get pregnant?
Dr. Shah recommends waiting 3–6 months after laparoscopic myomectomy before attempting IVF or natural conception. This healing period allows the uterine scar to fully consolidate. For hysteroscopic myomectomy (smaller submucosal fibroids removed through the cervix), the wait is typically 1–2 months. Attempting pregnancy too early after myomectomy carries a small but real risk of uterine rupture during pregnancy.
My doctor said my fibroid is 5cm — should I be worried?
Not necessarily. A 5cm subserosal fibroid sitting on the outside of your uterus with no cavity involvement may require nothing more than regular monitoring. A 5cm intramural fibroid that is pressing into the uterine cavity is a different matter — surgery may be warranted before fertility treatment. The size alone does not tell us enough. The location relative to the uterine cavity, assessed on ultrasound or MRI, is the deciding factor.
Can fibroids cause recurrent miscarriage?
Yes — submucosal fibroids are a recognised cause of recurrent implantation failure and early miscarriage. They alter the uterine environment in ways that impair embryo implantation and early placentation. If you have had two or more miscarriages and you have a submucosal fibroid, it should be removed and a hysteroscopy performed to ensure the cavity is clear before the next pregnancy attempt.
What is the difference between fibroids and adenomyosis?
Fibroids are distinct muscular growths — separate from the uterine tissue. Adenomyosis is when the uterine lining (endometrium) grows into the muscular wall of the uterus itself. The uterus becomes bulky and thickened throughout — it is not a discrete mass. Fibroids can be removed surgically. Adenomyosis cannot be excised in the same way. The two conditions frequently coexist — a woman can have both simultaneously — which is why both must be specifically assessed.
Will my fibroids grow back after myomectomy?
Fibroids can recur after myomectomy — particularly when multiple fibroids were present at the time of surgery. The recurrence rate is approximately 10–15% at 5 years. This is higher for women with multiple fibroids (more than 3) at the original surgery. Dr. Shah discusses recurrence risk as part of pre-surgical counselling, and monitors post-operative scans to detect any recurrence early.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026