Fresh IVF Cycle & Embryo Transfer in Ahmedabad
Request a Free Callback
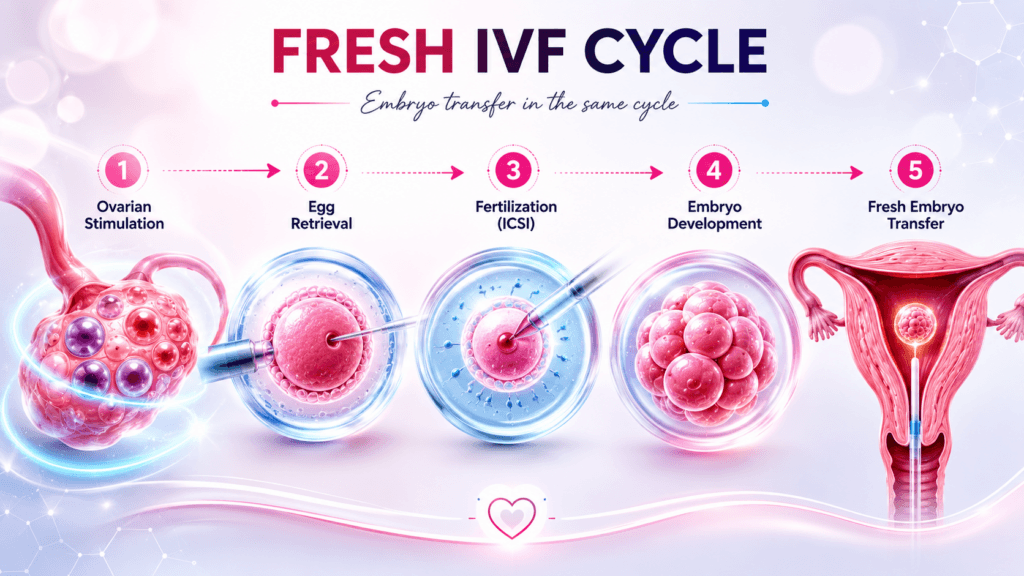
Fresh IVF Cycle in Ahmedabad — Stimulation, Retrieval, Transfer in One Continuous Journey
There is a growing tendency in IVF to default every patient to a freeze-all strategy — freeze all embryos, transfer in a later cycle. It is not wrong. In specific clinical situations — high responders, elevated progesterone, PGT-A planned — it is clearly the better choice. But it is not the universal answer, and applying it universally does not serve every patient.
A fresh IVF cycle — where the embryo is transferred back to the uterus in the same cycle it was created — remains the gold-standard path for the right candidate. No waiting cycle. No additional endometrial preparation. No thaw procedure. Continuous, uninterrupted from stimulation to potential pregnancy. For women with normal ovarian response, a good endometrial lining, and normal progesterone levels at the time of trigger, the fresh transfer success rate is excellent — and the overall pathway is faster and less expensive.
At Wellspring IVF, Dr. Pranay Shah decides the fresh vs frozen strategy based on your specific clinical picture at each monitoring scan — not a default policy set before stimulation begins. Progesterone on trigger day, endometrial thickness and pattern, OHSS risk assessment, and embryo number all inform the decision in real time. This page explains everything about how a fresh IVF cycle works, who it is best suited for, and what makes Wellspring IVF’s approach to protocol selection different.
Fresh IVF Cycle — The Right Choice for the Right Patient
Not every patient needs to freeze all embryos and wait an extra 6–8 weeks. For the optimal fresh candidate, this path is faster, equally effective, and more cost-efficient.
Fresh IVF Cycle Overview
Key parameters, protocols, and selection criteria at a glance
| Parameter | Clinical Guidelines & Details |
|---|---|
| What Is a Fresh Cycle | An IVF cycle in which the embryo is transferred back to the uterus in the same stimulation cycle it was created — no freezing required. |
| Total Duration | Approximately 3–4 weeks from Day 1 of stimulation to embryo transfer. Pregnancy test 14 days after transfer. |
| Key Advantage | Continuous — no waiting cycle. Fewer appointments than a freeze-all + FET strategy. Lower overall lab cost when freezing is not clinically needed. |
| Best Candidate | Women under 38 with normal ovarian reserve, normal progesterone on trigger day, 2–5 embryos only, no OHSS risk, no PGT-A planned. |
| Not Ideal For | High responders (OHSS risk), elevated progesterone on trigger day (>1.5 ng/mL), PGT-A required, severe thin endometrium during stimulation. |
| Stimulation Protocols | Antagonist (most common), Long Agonist, Short/Flare, Mini-IVF — Dr. Shah selects based on AMH, AFC, age, and diagnosis. |
| Trigger Options | hCG trigger (standard) or GnRH agonist trigger (for OHSS-risk patients even in fresh cycles — followed by luteal support). |
| Transfer Day | Day 3 (cleavage) or Day 5 (blastocyst) — Dr. Shah’s default is Day 5 blastocyst where embryo number permits. |
| Success Rate | 60–75% per cycle for women under 35 with good ovarian reserve. Comparable to FET in the right candidate. |
| Embryos Not Transferred | Surplus good-quality embryos are vitrified (frozen) for future FET cycles — not discarded. |
| Consultation | Selection discussed at your first consultation. Call 9099946050 to plan your journey. |
Who Is a Fresh IVF Cycle Best For? — The Clinical Selection Criteria
Ideal Candidates for Fresh Embryo Transfer
- Age under 38 with good ovarian reserve (AMH ≥1.2 ng/mL): Younger women with adequate reserve are more likely to produce embryos of sufficient quality to justify a fresh transfer without the benefit of genetic testing. The endometrium during stimulation is typically receptive when progesterone is normal. Age is the most powerful predictor of embryo chromosomal integrity — the case for PGT-A (and therefore freeze-all) is stronger in women over 38.
- Normal serum progesterone on trigger day (≤1.5 ng/mL): This is the single most important biochemical gate for fresh transfer. Elevated progesterone (>1.5 ng/mL) on the day of trigger injection indicates premature luteinisation — the endometrium has begun its secretory transformation ahead of schedule. The embryo and endometrium are no longer in synchrony. Fresh transfer in this setting has significantly reduced implantation rates. When progesterone rises above threshold, Dr. Shah converts to a freeze-all strategy regardless of embryo quality.
- Good endometrial development — trilaminar pattern, ≥8mm thickness: The endometrium must show a trilaminar (triple line) pattern on transvaginal ultrasound and reach at least 8mm thickness before transfer. In some patients, the stimulation hormones themselves thin the lining — a thin endometrium during a fresh cycle is an indication to freeze and transfer in a natural or medicated FET cycle instead.
- Moderate ovarian response — 3–12 eggs retrieved: Women who produce a moderate number of eggs are the ideal fresh candidates. High responders (>15 eggs) carry OHSS risk — elevated oestrogen levels during stimulation create a hypercoagulable, pro-inflammatory uterine environment that impairs implantation. Low responders (1–3 eggs) can still have fresh transfers, though Dr. Shah discusses the embryo number and quality in detail before making the decision.
- No plan for PGT-A / chromosomal testing: PGT-A (Preimplantation Genetic Testing for Aneuploidies) requires embryos to be biopsied at the blastocyst stage and sent to a genetics lab — a process that takes 2–3 weeks. This makes a fresh transfer in the same cycle impossible. If Dr. Shah recommends PGT-A (recurrent miscarriage, age >38, recurrent implantation failure), a freeze-all strategy is mandatory.
- Younger couples where time-to-pregnancy is a priority: For couples under 35 with no identified complicating factor, a successful fresh cycle delivers a pregnancy result in approximately 5–6 weeks from stimulation start. A freeze-all + FET strategy adds 6–10 weeks of waiting. Where the clinical picture supports fresh transfer, Dr. Shah does not impose unnecessary delay.
When Dr. Shah Converts to Freeze-All (Fresh Transfer Avoided)
- Progesterone >1.5 ng/mL on trigger day: Premature luteinisation — the most common reason for unexpected freeze-all. The endometrium is out of sync with the embryo. Fresh transfer would significantly reduce the chance of implantation. Freeze all good-quality embryos and transfer in a subsequent natural or medicated FET cycle with optimal endometrial preparation.
- High responder — OHSS risk (>15 follicles, oestradiol >4,000 pg/mL): Ovarian Hyperstimulation Syndrome (OHSS) is rare but serious. In high-risk patients, a GnRH agonist trigger replaces the hCG trigger — this eliminates OHSS risk but significantly reduces the luteal phase support available for fresh transfer. Freeze-all is mandatory in agonist-triggered cycles for OHSS prevention. FET in the next cycle carries no OHSS risk and gives the best outcome.
- Thin endometrium (<7mm) or poor trilaminar pattern: The embryo has nowhere optimal to implant. A frozen embryo transfer in the next cycle, with dedicated endometrial preparation using oestrogen supplementation (with or without hysteroscopy if a structural cause is found), gives a significantly better implantation environment.
- PGT-A planned (recurrent miscarriage, age >38, recurrent IVF failure): Genetic biopsy results require 2–3 weeks from the genetics laboratory. Freeze-all is non-negotiable in PGT-A cycles. Only euploid (chromosomally normal) embryos are transferred — and only after the result is confirmed. Guide: Recurrent Miscarriage at Wellspring IVF
- Severe male factor with ICSI and high DFI: In cases of very high sperm DNA fragmentation (DFI >40%), the embryo quality signal may only become clear at the blastocyst stage. Waiting for blastocyst formation and then vitrifying the best embryo for a subsequent FET often delivers better outcomes than rushing to a fresh Day 3 or Day 5 transfer before quality assessment is complete.
Stimulation Protocols — How Dr. Shah Personalises Your IVF
GnRH Antagonist Protocol
Best For: Most patients — first-line choice for normal and high responders. PCOS patients.
Stimulation Duration: Day 2–12.
Trigger Type: hCG trigger or GnRH agonist trigger.
Long GnRH Agonist Protocol
Best For: Endometriosis, adenomyosis, fibroids.
Stimulation Duration: Down-regulation 14–21 days.
Trigger Type: hCG trigger.
Short / Flare Protocol
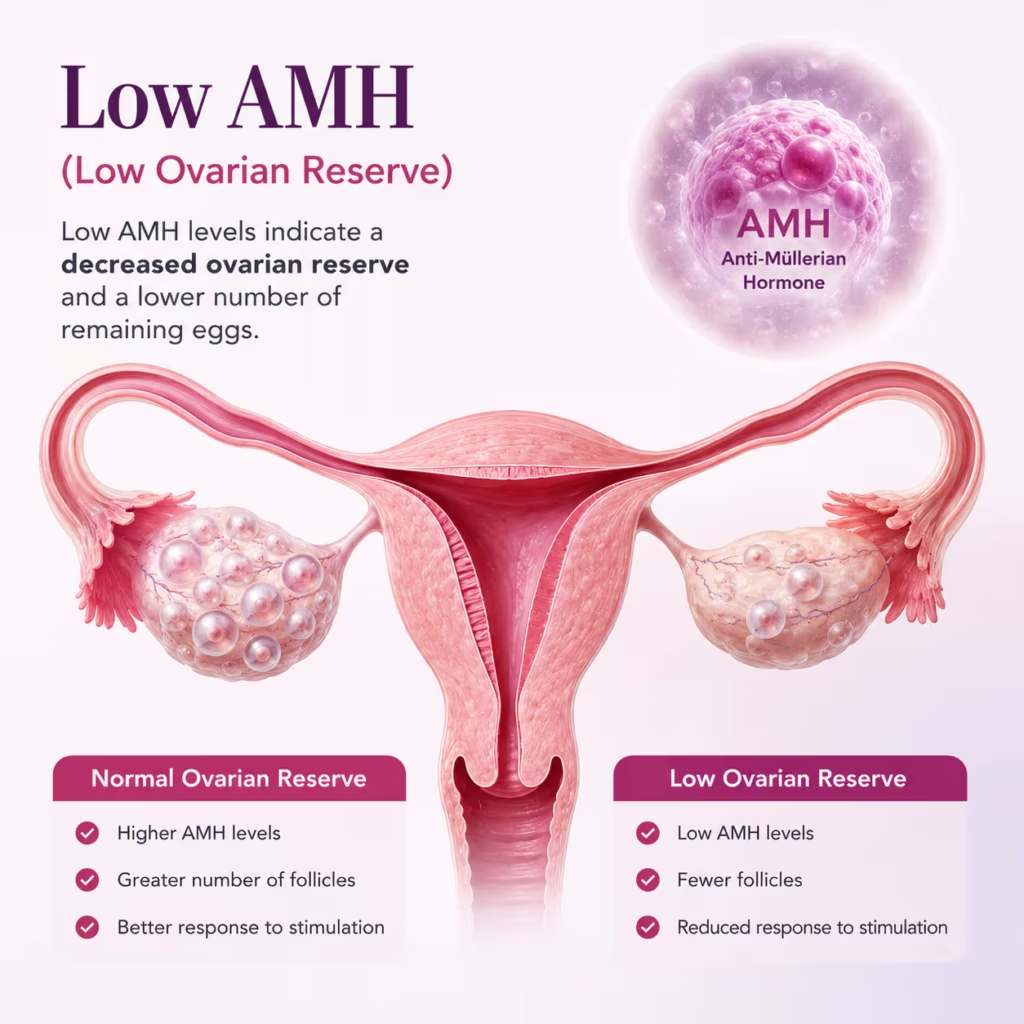
Best For: Poor ovarian reserve, low AMH.
Stimulation Duration: 9–12 days total.
Trigger Type: hCG trigger.
Mini-IVF / Minimal Stimulation
Best For: Very low AMH, poor responders.
Stimulation Duration: 5–8 days only.
Trigger Type: hCG trigger or natural LH surge monitoring.
Dr. Shah’s Protocol Selection Principles:
The antagonist protocol is the modern first choice for most patients — shorter, flexible, with the option to switch to agonist trigger if OHSS risk develops. The long agonist protocol remains superior for endometriosis and adenomyosis — the extended down-regulation reduces endometrial and ovarian inflammatory activity before stimulation begins. Poor responders often benefit from the micro-flare — the initial agonist dose creates a natural FSH surge that supplements the injected FSH, maximising the response from a limited follicle pool. Mini-IVF is not a cost-cutting measure — it is a medically indicated choice for specific patients where conventional stimulation would not materially increase egg yield but would increase side effects.
Watch Our Fresh IVF Cycle Treatment VS Frozen Cycle Video
Learn how a fresh IVF cycle works, when fresh embryo transfer may be recommended, and how it compares with frozen embryo transfer.
What You Will Learn
Understand the benefits, limitations, and success factors of a fresh IVF cycle.
- Fresh IVF cycle process
- Fresh embryo transfer timing
- Success factors and considerations
- Fresh vs frozen IVF comparison
The Fresh IVF Cycle — Complete Day-by-Day Timeline
Pre-Cycle Baseline Assessment
- Transvaginal ultrasound: antral follicle count (AFC), uterine cavity check, both ovaries scanned for cysts
- Blood tests: Day 2 FSH, LH, Estradiol (E2), AMH confirmation if not recent
- Protocol confirmed: medication type, starting dose, injection schedule, calendar
- Nurse appointment: injection technique training — most patients self-administer at home
- Baseline progesterone confirmed normal — stimulation contraindicated if elevated
First FSH/HMG Injection — Stimulation Starts
- Gonadotropin injections begin: Gonal-F, Puregon, or Menopur (based on protocol)
- Subcutaneous injection — abdomen or thigh. Takes <2 minutes. Most patients report minimal discomfort
- Dose: individualised to your AMH and AFC. Never the same number for every patient
- Continue daily until trigger night (Day 10–14 depending on response)
First Monitoring Scan + Antagonist Added
- Transvaginal scan: follicle count in each ovary, lead follicle diameter measurement
- Blood test: Estradiol (E2) — confirms follicles are producing hormones as expected
- GnRH antagonist starts (Cetrotide or Orgalutran) — prevents premature LH surge
- Dose adjustment: Dr. Shah reviews result and modifies FSH dose if needed
- This is a working day scan — appointment takes approximately 30 minutes
Continued Monitoring — Follicle Growth Tracking
- Scan every 2–3 days from Day 6 onwards — follicle diameter measured individually
- Target: lead follicles reaching 17–20mm diameter for mature egg
- Endometrial thickness and pattern checked at every scan
- Estradiol continues to rise — confirms growing follicles are healthy and producing hormones
- Progesterone monitored closely approaching trigger day — key decision point
- Most patients have 2–3 monitoring scans total during stimulation
Trigger Injection — Final Egg Maturation
- When ≥3 lead follicles reach 17–20mm AND endometrium ≥8mm trilaminar: trigger decision made
- Progesterone checked: if ≤1.5 ng/mL → fresh transfer proceeds. If elevated → freeze-all decision
- hCG trigger (Ovitrelle): standard for normal responders. Timed precisely 34–36 hours before OPU
- GnRH agonist trigger (Lupride/Buserelin): used if OHSS risk detected — prevents OHSS
- No sexual intercourse from trigger night to egg retrieval
- Partner’s semen sample appointment confirmed for OPU morning
Egg Retrieval — Ovum Pick-Up (OPU)
- Performed under intravenous sedation — patient is fully comfortable, no general anaesthesia
- Dr. Shah performs every retrieval personally — transvaginal ultrasound-guided follicle aspiration
- Duration: 15–25 minutes depending on follicle number and access
- Embryologist receives follicular fluid in the adjacent laboratory immediately — eggs identified, counted, graded
- Recovery: 2–3 hours in the clinic. Light spotting and mild cramping normal for 1–2 days
- Discharge criteria: stable observations, oral intake tolerated, responsible adult escort
- Average mature eggs retrieved at Wellspring IVF: 8–14 in normal responders
ICSI — Sperm Injection & Fertilisation
- Partner’s semen sample collected same morning — processed by swim-up and density gradient
- Mature eggs (MII oocytes) identified and prepared for ICSI
- ICSI: embryologist selects best single sperm under 400× magnification, injects into each mature egg
- PICSI or MACS added if sperm DFI is elevated — hyaluronan-binding selection before injection
- Fertilisation assessment next morning (Day 1 post-OPU): 2-pronucleate embryos confirm fertilisation
- Fertilisation report communicated to couple: typically 70–80% of mature eggs fertilise
Embryo Development — Day 1 to Day 5
- Embryos cultured in precision incubators: 37°C, 6% CO₂, 5% O₂, HEPA-filtered air
- Day 2 (4-cell), Day 3 (6–8 cell): cleavage stage assessment — fragmentation, symmetry
- Day 4: compaction — embryos forming morula
- Day 5: blastocyst — inner cell mass visible, trophectoderm expanding
- Gardner blastocyst grading: expansion grade (1–6) + ICM quality (A/B/C) + TE quality (A/B/C)
- Target: Grade 4AA, 5AA, or 6AA blastocyst for transfer
- Surplus good-quality blastocysts vitrified (frozen) for future FET cycles
Embryo Transfer — The Final Step
- Best-quality embryo selected for transfer — confirmed by Dr. Shah and embryologist together
- Bladder comfortably full (aids ultrasound visualisation) — no sedation required
- Soft catheter passed through cervix under abdominal ultrasound guidance
- Embryo loaded in a tiny droplet of culture medium — deposited in upper uterine cavity
- Procedure duration: 5–10 minutes. Mild uterine cramping possible — resolves quickly
- Rest for 30–45 minutes post-transfer. Return to light activity same evening
- Luteal support begins: progesterone pessaries (Crinone/Utrogestan) + oestrogen as per protocol
- eSET (elective Single Embryo Transfer): Dr. Shah’s standard — reduces twin risk without reducing success
Luteal Phase — Progesterone Support & the Wait
- Progesterone pessaries 200mg BD or TID — vaginally. Do not stop without Dr. Shah’s instruction
- Avoid: hot baths, strenuous exercise, NSAIDs (ibuprofen). Light activity is fine
- Symptoms during the 2WW: mild spotting (implantation or progesterone effect), breast tenderness, bloating — all normal
- Home pregnancy tests: Dr. Shah recommends waiting for the blood beta-hCG — urine tests can mislead
- WhatsApp access to the Wellspring IVF team for any questions during the wait
Beta-hCG Blood Test — Pregnancy Confirmation
- Serum beta-hCG measured 14 days after transfer — the definitive pregnancy test
- Positive (>25 mIU/mL): progesterone support continued. First ultrasound at 6–7 weeks gestation
- Negative: Dr. Shah consultation within 48 hours — review cycle, adjust protocol, plan next step
- Frozen embryos from this cycle: available for FET attempt. No repeat stimulation needed
- Repeat beta-hCG 48–72 hours if borderline result — doubling time confirms viable pregnancy
Fresh vs Frozen Embryo Transfer — The Objective Comparison
| Factor | Fresh Transfer | Frozen (FET) |
|---|---|---|
Total cycle time | 3–4 weeks stimulation to result | 6–10 weeks (stimulation + freezing + prep cycle + FET) |
Endometrium quality | May be suboptimal — stimulation hormones can affect lining | Fully prepared in a dedicated, unstimulated cycle |
OHSS risk | Present — especially in high responders | Zero — stimulation is complete |
Progesterone level | Must be ≤1.5 ng/mL on trigger day — can rise unexpectedly | Not a limiting factor — progesterone is controlled |
Cost | Lower — no cryopreservation or thaw fees | Higher — adds vitrification, storage, and FET cycle cost |
PGT-A compatible | No — genetic testing requires freeze and lab time | Yes — only option with PGT-A |
Best success rate evidence | Normal responders, normal progesterone, good lining | High responders, elevated progesterone, OHSS risk, PGT-A |
Emotional journey | Shorter — fewer appointments, quicker result | Longer — more planning cycles, waiting periods |
Dr. Shah’s decision point | Trigger day progesterone + endometrial assessment | Any of: OHSS risk, prog >1.5, PGT-A, thin lining |
The Evidence on Fresh vs Frozen Success Rates:
Multiple large RCTs (including the FRESH trial) show: in normal responders with normal progesterone, fresh transfer success rates are equivalent to FET. In high responders, freeze-all strategies show significantly higher live birth rates due to the OHSS-free, fully prepared endometrium. The conclusion: freeze-all is not universally better — it is selectively better. Dr. Shah applies the evidence to your specific clinical picture, not to a clinic-wide protocol preference.
For the complete frozen embryo transfer guide: Frozen Embryo Transfer (FET) — Wellspring IVF
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Day 3 vs Day 5 Transfer — Cleavage vs Blastocyst
Day 5 Blastocyst Transfer — Dr. Shah’s Preferred Default
Culturing to blastocyst (Day 5) allows natural selection — embryos with poor developmental potential arrest before reaching blastocyst, eliminating them from the transfer pool without invasive testing. The result: only embryos with proven developmental capacity are transferred. Blastocyst implantation rates: 45–55% per transfer, significantly higher than Day 3 cleavage embryo rates of 25–35%. The synchrony between a Day 5 embryo and the uterine lining on Day 5 post-trigger is also physiologically optimal.
When Day 3 Transfer Is Indicated
Fewer than 3 fertilised embryos (extended culture risks losing all embryos). Previous cycles with complete blastocyst arrest (embryos arrested every time in culture). Patient age with very few eggs (every embryo has value — don’t risk arrest in culture). In these cases, Day 3 transfer ‘saves’ embryos that might have arrested in the lab but would have had the natural uterine environment for further development. The uterus is the better incubator for borderline embryos.
Wellspring IVF blastocyst conversion rate
50–65% of fertilised eggs that begin culture reach a full blastocyst by Day 5. This is a direct reflection of embryo quality and lab conditions. Our HEPA-filtered, VOC-controlled laboratory environment is specifically designed to maximise blastocyst conversion from the available cohort.
The arrest conversation
The most emotionally difficult outcome: all embryos arrest in culture before reaching Day 5. No transfer. This outcome — while distressing — provides critical diagnostic information: it confirms embryo developmental failure as the mechanism of the problem. Dr. Shah uses this information to adjust protocol, investigate DFI, and plan the next cycle. It is information that a Day 3 transfer would not have revealed.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Medications in a Fresh IVF Cycle — What You Will Be Taking and Why
Understanding your medication list removes much of the anxiety of starting IVF. Here is a complete reference table for a standard antagonist protocol fresh cycle:
| Medication | Type | When | Purpose |
|---|---|---|---|
Gonal-F / Puregon / Menopur | Recombinant FSH or FSH+LH | Days 2–12 | Stimulates ovarian follicles to grow and mature multiple eggs |
Cetrotide / Orgalutran | GnRH Antagonist | Days 5–6 until trigger | Prevents premature LH surge — stops spontaneous ovulation before retrieval |
Ovitrelle (hCG 250mcg) | Trigger injection | Single dose — 34–36h before OPU | Final maturation of eggs — completes meiosis. The precise timing is critical |
Lupride / Buserelin | GnRH Agonist trigger | Alternative trigger — OHSS risk cases | Triggers ovulation without hCG effect — eliminates OHSS. Requires luteal rescue |
Crinone gel / Utrogestan | Progesterone | From day after OPU | Supports the uterine lining (luteal phase). Prevents early period. Continue until 12 weeks if pregnant |
Estradiol valerate | Oestrogen supplement | Day after OPU if thin lining | Supports endometrial thickness in luteal phase |
Prednisolone / Dexamethasone | Corticosteroid (selected cases) | Days 1–OPU or post-transfer | Reduces NK cell activity in selected immunological implantation failure cases |
Low-dose Aspirin (75mg) | Antiplatelet | From stimulation start | Improves endometrial blood flow in selected patients with thin lining history |
LMWH (Clexane 40mg) | Anticoagulant | From trigger day if APS/thrombophilia | Prevents placental thrombosis in patients with antiphospholipid syndrome |
Medication Cost Transparency:
Stimulation medications (FSH/HMG injections) are the largest variable cost in IVF. Total medication cost for a standard fresh antagonist cycle: approximately ₹25,000–₹70,000 depending on the starting dose and total stimulation days. Low AMH patients requiring higher doses for longer duration will be at the upper end. Dr. Shah estimates your medication cost at the baseline appointment based on your AMH and AFC — before the first injection is purchased. Medications are prescription items — always purchased from licensed pharmacies. Do not purchase IVF medications without a prescription.
Talk to Dr. Shah About Cavity Optimisation
Ovarian Hyperstimulation Syndrome (OHSS) — Risk, Recognition, Prevention
- What is OHSS? Ovarian Hyperstimulation Syndrome occurs when the ovaries over-respond to stimulation — producing too many follicles, which then over-produce oestrogen and vascular endothelial growth factor (VEGF). Fluid leaks from blood vessels into the abdomen (and in severe cases, the chest). Range: mild (bloating, discomfort) to severe (respiratory compromise, thrombosis) — severe OHSS is rare (<1%) when managed properly.
- Who is at risk? PCOS patients (multiple small follicles — high baseline AFC). AMH >4.0 ng/mL. Previous OHSS. Young women with high AFC (>20 total follicles). Oestradiol rising >300 pg/mL per follicle on Day 8–10 of stimulation.
- Early warning signs to report immediately: Severe abdominal bloating or pain. Nausea and vomiting. Reduced urine output (dark urine). Difficulty breathing. Weight gain >2kg in 24 hours. These are indications to contact the Wellspring IVF team immediately — 9099946050.
- Prevention — Dr. Shah’s protocol: Coasting (reducing FSH dose when oestradiol rises rapidly). GnRH agonist trigger instead of hCG (when OHSS risk identified mid-cycle — eliminates OHSS but requires freeze-all of all embryos). Cabergoline (0.5mg daily for 7 days after trigger) reduces VEGF-mediated fluid shift in moderate-risk patients. Freeze-all strategy: removing the fresh transfer removes the hCG of pregnancy that would otherwise sustain and worsen OHSS.
- Mild OHSS is manageable at home: High protein diet (eggs, dahl, paneer — helps maintain oncotic pressure). Oral hydration with electrolyte drinks (ORS, coconut water). Rest. Avoid strenuous activity. Paracetamol for discomfort — NOT ibuprofen or diclofenac (NSAIDs). Daily weight monitoring. Clinic review if weight gain >1kg/day.
“I do not believe in a freeze-all default. I believe in the right decision for the right patient, made with the right information. When a woman under 37 has a good response, a normal progesterone on trigger day, a beautiful trilaminar endometrium at 9mm, and three high-quality blastocysts — why make her wait another 6 weeks and pay for a FET cycle she does not clinically need? The fresh cycle, in the right patient, is elegant. The embryo goes home in the same continuous journey it was created in. That is the biology working the way it was designed to work.”
Frequently Asked Questions
How do I know if a fresh cycle is right for me, or if I should freeze all embryos?
This decision is made in real-time during your cycle — not at your first appointment. At the trigger day monitoring (approximately Day 12), Dr. Shah checks: (1) your serum progesterone — if >1.5 ng/mL, fresh transfer is cancelled and all embryos are frozen. (2) Your endometrial thickness and pattern. (3) Your ovarian response — if OHSS risk is high. If all three are favourable, fresh transfer proceeds. If any one raises a red flag, freeze-all protects your embryos and your outcome.
How many injections will I need during a fresh IVF cycle?
For a standard antagonist protocol, approximately 10–15 injections in total: FSH/HMG daily for 8–12 days, GnRH antagonist for 5–6 days, a single trigger injection, then progesterone pessaries (not injections) for luteal support. The FSH injections are subcutaneous — most patients self-administer confidently within 2 days of the nursing training session. The needles are very small. For a long protocol: add 14–21 days of agonist nasal spray or injections before stimulation.
Does a fresh IVF cycle hurt?
The injections: minimal discomfort — subcutaneous needles in the abdomen are well tolerated by most patients. Some mild bruising at injection sites is common. The egg retrieval: performed under IV sedation — you are asleep and feel nothing. Post-retrieval: mild cramping for 1–2 days, similar to period pain. Paracetamol is adequate. The embryo transfer: no sedation, no pain — a soft catheter through the cervix. Most patients compare it to a smear test. The procedure takes 5–10 minutes.
What happens to embryos that are not transferred in a fresh cycle?
All surplus good-quality embryos — those that are not transferred in the fresh cycle — are vitrified (frozen) and stored at Wellspring IVF. These embryos remain yours and are available for future Frozen Embryo Transfer (FET) cycles. If the fresh transfer succeeds and you want a second child later, you may have frozen embryos available — eliminating the need for another full stimulation cycle. Frozen embryos can be stored for years. Full FET guide: Frozen Embryo Transfer at Wellspring IVF
What is the success rate of a fresh IVF cycle at Wellspring IVF?
For women under 35 with good ovarian reserve, the fresh transfer success rate at Wellspring IVF is approximately 60–75% per cycle. This depends on: your age, your embryo quality, your endometrial response, and whether Dr. Shah’s fresh vs frozen decision framework supports fresh transfer at your trigger day. The overall Wellspring IVF success rate (across all protocols and patient groups) is 70%+. Dr. Shah gives you a personalised probability at your first consultation — not a generic clinic average.
Can I work during a fresh IVF cycle?
Yes — most patients continue working throughout stimulation. You will need to attend the clinic on approximately 3–4 weekday mornings for monitoring scans (each takes 30 minutes). Egg retrieval day requires a full day off — sedation means you cannot drive. Embryo transfer day: many patients take a half-day and return to light work the same evening. The 2-week wait: normal activity is fine. Physical exertion and hot environments should be avoided from trigger day onwards.
How soon after egg retrieval is the embryo transferred in a fresh cycle?
For a Day 5 blastocyst transfer (Dr. Shah’s default): 5 days after egg retrieval. Egg retrieval on Day 14 of the cycle → blastocyst transfer on Day 19–20. For a Day 3 cleavage embryo transfer (when indicated): 3 days after retrieval. From the first stimulation injection to the embryo transfer: approximately 3 weeks.
What should I do and avoid during the 2-week wait after embryo transfer?
Continue: all prescribed progesterone and oestrogen medications exactly as directed. Light walking. Normal diet (high protein, avoid raw or unpasteurised foods). Normal sleep routine. Paracetamol for any pain (not ibuprofen). Avoid: hot baths, saunas, vigorous exercise, alcohol, smoking, heavy lifting. Do not stop progesterone even if you have spotting — spotting is common in early pregnancy and does not indicate failure. Wait for the blood beta-hCG on Day 14 post-transfer — do not rely on home urine pregnancy tests, which can mislead in both directions.
Related Conditions & Treatments
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026