No Surgery
Simple, minimally invasive procedure
If you have been trying to conceive for some time and your doctor has suggested fertility treatment, IUI — Intrauterine Insemination — is very often the recommended first step. And for good reason. It is simple, it is gentle, it is effective for the right patients, and it gives your body the best possible assisted chance to achieve what it is designed to do naturally.
IUI works by placing a carefully prepared, highly concentrated sample of the partner’s (or donor’s) sperm directly inside the uterus — right at the time of ovulation — using a soft, thin catheter. No surgery. No anaesthesia. No needles inside the body. The sperm is placed in the optimal location at the optimal moment, giving it a significant head start on the natural journey to fertilisation — which still occurs naturally inside the fallopian tube.
At Wellspring IVF & Women’s Hospital, IUI is performed under the direct supervision of Dr. Pranay Shah with precise ovulation monitoring via serial transvaginal ultrasound scans and timed HCG trigger injection. The difference between a well-monitored IUI and a poorly timed one is significant. Precision is everything.

Many patients are surprised by how straightforward an IUI cycle is. There is no egg retrieval. No embryo culture. No laboratory fertilisation. The entire cycle follows your natural menstrual calendar, gently guided by monitoring and mild medication.
Your IUI cycle begins on Day 1 to Day 2 of your menstrual period. A baseline transvaginal ultrasound is performed to assess uterine lining thickness, resting antral follicles in both ovaries, and to confirm no residual cysts from the previous cycle. Baseline blood tests (Day-2 FSH, LH, oestradiol) are taken if not already available. The IUI cycle plan is confirmed at this visit.
In most IUI cycles, mild stimulation medications encourage the growth of 1–3 dominant follicles. Options include oral Clomiphene Citrate or Letrozole (tablet form), or low-dose injectable Gonadotrophins (FSH/LH). The goal is controlled development of 1–2 dominant follicles — not the high-stimulation approach used in IVF. Natural (unstimulated) IUI is also performed in selected cases where ovulation is confirmed to be regular.
This is where Dr. Pranay Shah’s expertise makes the critical difference. Follicle growth is tracked via 2–3 transvaginal ultrasound scans during the stimulation phase. When the lead follicle reaches 18–22 mm in diameter — the mature, ovulation-ready size — the trigger injection is given. Precise follicle monitoring is what separates a well-timed IUI from a poorly timed one. Endometrial thickness and trilaminar pattern are also assessed at this stage (target: ≥ 8mm).
When follicle maturity is confirmed, a single HCG (Human Chorionic Gonadotropin) trigger injection is administered. This injection precisely triggers the final maturation of the egg and initiates the ovulation process approximately 36–40 hours later. The IUI procedure is then scheduled 36–38 hours after the trigger — timed to coincide exactly with the natural ovulation window. This is the most time-critical step in the entire IUI cycle.
On the morning of the IUI procedure, the male partner provides a semen sample (or a frozen donor/partner sample is thawed). This sample undergoes the sperm washing process — explained below. The wash typically takes 60–90 minutes. The result: a small volume (0.3–0.5 mL) of highly concentrated, highly motile, sterile sperm in culture medium — ready for direct uterine placement.
You lie on the examination table as for a standard gynaecological check-up. A thin, flexible catheter is gently passed through the cervix — no dilation required in most cases. The washed sperm sample is slowly injected into the uterine cavity. The catheter is withdrawn. Mild cramping may be felt briefly. You rest for 10–15 minutes post-procedure and then return to your normal daily activities. No bed rest. No special restrictions. No anaesthesia.
Vaginal progesterone pessaries (Crinone / Utrogestan) are prescribed after IUI to support the uterine lining and create a receptive environment for implantation. These are continued for 14 days. The two-week wait can be emotionally challenging — Dr. Shah’s team is available by WhatsApp for any questions. A blood Beta-hCG test is performed 14 days after IUI, not a urine test which can be unreliable at this early stage.
A positive result is confirmed by a rising hCG level (repeated 48 hours later) and then a confirmatory ultrasound at 6–7 weeks to see the fetal heartbeat. A negative result triggers a dedicated consultation with Dr. Shah — to review the cycle data, discuss what can be optimised, and plan the next step: another IUI cycle with protocol adjustment, or transition to IVF. A failed IUI cycle is never simply ‘try again’ — it is a data point that informs the next decision.
Learn how IUI treatment works, when it may be recommended, and what couples can expect during the process.
This video explains how IUI treatment works, who may benefit from it, and what couples can expect during the fertility treatment process.







| Condition | Why IUI Is Not Indicated — and What Is Recommended Instead |
|---|---|
| Bilateral blocked fallopian tubes | Sperm cannot reach the egg even if placed in the uterus — IVF is required |
| Severe male factor (post-wash TMC < 2M) | Too few sperm for IUI to reliably succeed — ICSI is the appropriate treatment |
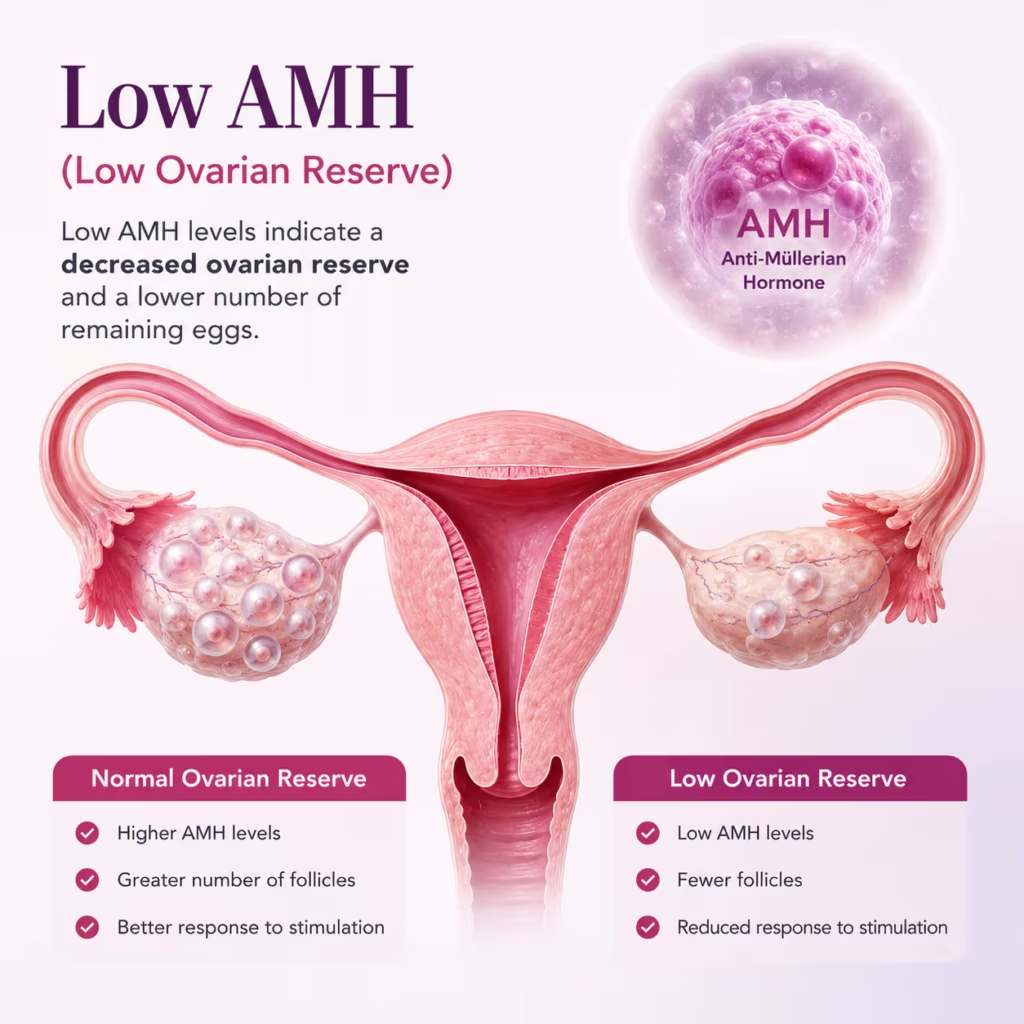
| Severe diminished ovarian reserve / very low AMH | IVF with controlled stimulation for low AMH case is more appropriate to maximise the chance from limited egg supply |
| Age > 38 + history of failed IUI cycles | IVF should be prioritised — time is a critical factor, and IUI delays the more effective option |
| Hydrosalpinx (fluid-filled blocked tube) | The fluid can impair implantation — laparoscopic treatment before IUI or direct IVF is recommended |
| Decision Factor | IUI | IVF/ICSI |
|---|---|---|
| Fallopian Tubes | At least one open, functional tube required | Tubes not required — fertilisation in laboratory |
| Sperm Quality | Post-wash TMC ≥ 5 million — mild male factor only | Any sperm quality including azoospermia with TESE |
| Egg Retrieval | No — ovulation occurs naturally | Yes — eggs retrieved under sedation |
| Fertilisation | Natural — inside fallopian tube | In laboratory — ICSI if sperm quality is poor |
| Success Rate per Cycle | 10–20% (diagnosis dependent) | 40–65% (age and diagnosis dependent) |
| Procedure Invasiveness | Minimal — 5 minutes, no anaesthesia | Moderate — OPU under sedation, embryo transfer |
| Cost per Cycle | Low — ₹10,000 procedure + medications | Higher — full cycle package at Wellspring IVF |
| Recommended First If | Unexplained infertility, mild male factor, PCOS, normal tubes | Failed IUI, blocked tubes, severe male factor, low AMH, age > 38 |
| Patient Profile | Per–Cycle Success Rate |
|---|---|
| Age < 35, unexplained infertility, good post-wash TMC Best-case IUI profile | 15–20% per cycle |
| Age < 35, PCOS with good ovulatory response With monitored cycles | 15–18% per cycle |
| Mild male factor, post-wash TMC 5–10 million | 10–15% per cycle |
| Age 35–38, any indication Declining egg quality is the primary variable | 8–12% per cycle |
| Age > 38, any indication IVF should be seriously considered | < 8% per cycle |
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.



Dr. Shah’s protocol recommendation The decision to proceed with a natural or stimulated cycle for your intrauterine insemination Ahmedabad protocol is entirely customized. This recommendation is based on your specific diagnosis, age, ovarian reserve, and previous fertility history. Because every couple’s journey is unique, there is no universal answer—precision timing and personal history guide our approach.
Wellspring IVF operates a strict no-hidden-costs philosophy. Every component of an IUI cycle is itemised and communicated clearly before you begin. The following breakdown reflects the standard IUI cycle cost structure:
The fixed ₹10,000 IUI procedure charge at Wellspring IVF covers:
IUI is generally well tolerated — similar to a cervical smear test. Most women describe mild cramping when the catheter passes through the cervix, which settles within a few minutes. No anaesthesia or sedation is required. You can drive yourself home and return to normal activity the same day.
The standard recommendation is 3-4 monitored, stimulated IUI cycles in good-prognosis patients (age under 35, open tubes, post-wash TMC above 5 million) before transitioning to IVF. Each failed cycle provides clinical data that informs both cycle optimisation and the decision to transition.
Potentially yes — if the other tube is confirmed open and functional, and the blocked tube is not causing additional problems such as a hydrosalpinx. A unilateral blocked tube reduces the number of ovulation events that can lead to IUI success. Dr. Shah will discuss the implications of your specific tubal finding at consultation.
Per-cycle IUI success rates at Wellspring align with international benchmarks: 10-20% per cycle depending on diagnosis and age. The most important number is your personalised expected rate calculated by Dr. Shah. Cumulative rates across 3 monitored cycles in good-prognosis patients: 35-50%.
Yes. IUI with donor sperm is performed at Wellspring IVF in full compliance with the ART (Regulation) Act 2021. Donor sperm from a licensed ART bank is used for single women, same-sex female couples, and couples where the male partner has no retrievable sperm.
A failed IUI cycle is reviewed by Dr. Pranay Shah at a dedicated follow-up consultation covering follicle response, endometrial lining, post-wash sperm quality, and timing precision. Dr. Shah then advises whether to proceed with another IUI cycle with protocol adjustment or transition to IVF. A failed IUI is never simply try again — it is a data point.
There are no strict restrictions after IUI. You can return to normal daily activities the same day. Avoid strenuous exercise and swimming for 48 hours. Avoid NSAIDs (ibuprofen, naproxen) during the luteal phase as they may interfere with implantation. Continue progesterone pessaries as prescribed