Uterine Polyps Treatment in Ahmedabad — Clearing the Ground for Implantation
Imagine your uterine cavity — the space where an embryo must land, attach, and build a placenta — as freshly prepared soil. Now imagine a pebble sitting in the middle of that soil. The seed cannot take root where the pebble sits.
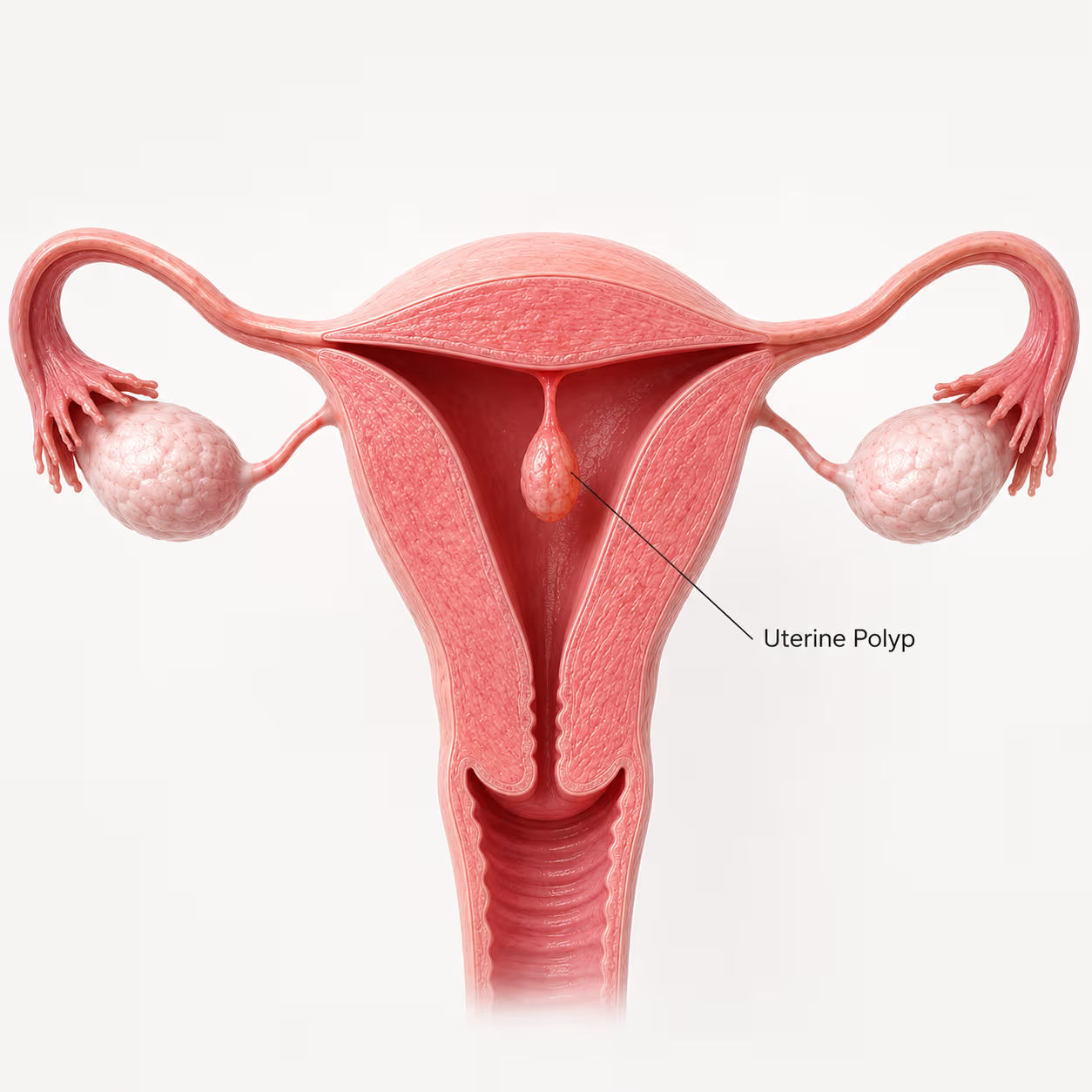
That is precisely how a uterine polyp interferes with implantation. A polyp is a soft, benign overgrowth of the uterine lining — attached to the inner wall of the uterus. It physically occupies space inside the cavity. And when an embryo is transferred into a uterus with a cavity polyp, the embryo's ability to implant is mechanically compromised — regardless of embryo quality, regardless of endometrial thickness, regardless of how perfect the protocol.
The particularly frustrating thing about uterine polyps is that they are entirely treatable. Unlike adenomyosis — which is diffuse and requires months of medical suppression — a polyp is a discrete, visible, physically removable structure. One procedure. No incisions. Day care. Done.
At Wellspring IVF & Women's Hospital, Dr. Pranay Shah performs operative hysteroscopy for polyp removal — passing a thin camera through the cervix into the uterine cavity under direct vision, identifying the polyp precisely, and removing it completely. No cuts. No hospital admission. The patient goes home the same day. And within 4–8 weeks — one menstrual cycle — the uterine cavity is restored and ready for IVF Treatment or natural conception.
The Most Fixable Cause of IVF Failure
Polyps are the one cause of implantation failure that is completely resolved in a single day-care procedure with no incisions and no recovery downtime.
Before any IVF cycle at Wellspring IVF, Dr. Shah confirms the uterine cavity is polyp-free. If a polyp is found — it is removed first.
Polyps are the one cause of implantation failure that is completely resolved in a single day-care procedure with no incisions and no recovery downtime.
Before any IVF cycle at Wellspring IVF, Dr. Shah confirms the uterine cavity is polyp-free. If a polyp is found — it is removed first.
What Are Uterine Polyps?
Uterine polyps — also called endometrial polyps — are localised overgrowths of the endometrial tissue that forms the inner lining of the uterus. They protrude inward into the uterine cavity, attached either by a thin stalk (pedunculated) or a broad base (sessile).

They are almost always benign — the malignancy risk in premenopausal women is approximately 0.3–3%. They range in size from 2–3mm (barely visible on standard ultrasound) to 5cm or more. Critically, size does not determine fertility impact.
A 3mm polyp sitting directly at the fundus (top of the uterine cavity — the preferred implantation site) causes more harm to IVF success than a 2cm polyp sitting low in the cavity away from the implantation zone.
Polyps are oestrogen-sensitive — they grow under oestrogen stimulation. This is why they are more common in: women with PCOS (high oestrogen state), obese women (adipose tissue produces oestrogen), women on tamoxifen therapy, and women approaching perimenopause. They can develop rapidly — a cavity that was clear on a scan 6 months ago may have a polyp today.
The Invisible Polyp — Why Standard Ultrasound Misses Them
A standard transvaginal ultrasound (TVS) can identify polyps in many cases — but small polyps (under 5–7mm) and flat (sessile) polyps are frequently missed on routine scanning. The endometrium must be assessed at the correct point in the menstrual cycle (proliferative phase — days 8–12) for polyps to be most visible.
The most accurate non-invasive assessment is Saline Infusion Sonography (SIS) — where saline is gently injected into the uterine cavity under ultrasound, causing the cavity walls to separate and making polyps (and other lesions) immediately visible against the fluid background. Dr. Shah uses SIS routinely before IVF cycles to confirm a clear cavity.
The definitive diagnosis is hysteroscopy — direct visual inspection of the uterine cavity. It also allows simultaneous polypectomy in the same procedure.
Types of Uterine Polyps — Location Determines Impact
Not all polyps carry the same fertility risk. Here is how different polyp types compare:
| Polyp Type | Location | Fertility Impact | Removal Urgency |
|---|---|---|---|
| Fundal Polyp | Top of uterine cavity (prime implantation zone) | HIGHEST — directly occupies the embryo's preferred landing site | Remove before any fertility treatment |
| Cornual Polyp | Near tubal openings (ostia) | HIGH — may obstruct tube + impair implantation | Remove before IVF; assess tube patency after |
| Mid-cavity Polyp | Central uterine cavity | HIGH — occupies main implantation area | Remove before IVF |
| Lower Segment / Cervical Polyp | Lower uterine segment or cervical canal | MODERATE — may not affect implantation directly but causes AUB and may obstruct embryo passage | Remove; less urgent for fertility |
| Multiple Polyps | Throughout cavity | HIGH COMBINED — even small multiple polyps cumulatively impair receptivity | Remove all before IVF |
How Uterine Polyps Cause IVF Failure — The Mechanism
The critical question for every IVF patient with a polyp: “Does this polyp need to come out before my transfer?” The answer, in almost every case where the polyp is within the uterine cavity, is yes — and here is precisely why:
Mechanical Obstruction — The IUD Effect
- The core problem: A polyp physically occupies space inside the uterine cavity — the space where the embryo must land and attach. When an embryo floats into the cavity after transfer, the polyp acts as a physical obstacle, preventing the embryo from making contact with healthy, receptive endometrium. This is functionally equivalent to the way a copper IUD prevents pregnancy — through physical interference with implantation.
- The size paradox: Even a 3–4mm polyp can prevent implantation if it sits at the fundus — the embryo’s preferred implantation site. Conversely, a 1cm polyp at the cervical end, away from the implantation zone, may have minimal impact. Location is the critical variable — not size.
- The evidence: A landmark 2001 study and subsequent meta-analyses consistently demonstrate that hysteroscopic polypectomy before IVF significantly improves pregnancy rates — with some studies showing a doubling of clinical pregnancy rates after polyp removal. The improvement is most pronounced for polyps within the uterine cavity (as opposed to cervical polyps).
Local Inflammatory Response — Disrupting Endometrial Chemistry
- The inflammatory mechanism: A polyp is not an inert physical object. It is metabolically active tissue that generates a localised inflammatory microenvironment within the uterine cavity. Studies demonstrate elevated levels of pro-inflammatory cytokines in the endometrial fluid of women with polyps — including IL-6, TNF-α, and VEGF — disrupting the molecular receptivity signals the embryo depends on for attachment.
- Endometrial receptivity markers: Polyps alter the expression of key implantation receptivity markers — including HOXA10, αvβ3 integrin (implantation marker), and leukemia inhibitory factor (LIF). These are the same molecular receptors disrupted in adenomyosis — but in polyps, the disruption is localised to the area around the polyp, rather than global.
- After removal: Complete polypectomy resolves the localised inflammatory environment within one menstrual cycle. After one period post-removal, endometrial cytokine levels normalise and receptivity markers recover. This is why a single menstrual cycle recovery before the next IVF transfer is both standard and sufficient.
Abnormal Uterine Bleeding — The Luteal Phase Problem
- The bleeding mechanism: Polyps cause abnormal uterine bleeding (AUB) through vascular fragility within the polyp’s surface vessels. Spotting between periods, heavy menstrual bleeding, and post-coital bleeding are the most common presentations.
- The fertility connection: In the context of IVF, mid-luteal or peri-implantation bleeding disrupts the hormonal environment at the critical implantation window — 5–9 days after ovulation or embryo transfer. Even minor bleeding during this window is associated with significantly reduced implantation rates in FET cycles.
- Silent polyps and failed cycles: Many women with polyps causing subtle intra-cavity bleeding never notice any symptoms — the bleeding is microscopic. But in an IVF cycle, this microscopic bleeding during the implantation window can be sufficient to prevent attachment. This is one reason polyps in otherwise ‘unexplained’ implantation failure cases are found on hysteroscopy after previous cycles showed ‘normal’ ultrasound scans.
What Our Patients Say
Real stories from real families who trusted us with their fertility journey

Ketan B.
2 months ago
I visited many doctors before, but this doctor was the one who correctly identified my issue and provided the right treatment. I finally started seeing real results after consulting them. Very knowledgeable, attentive, and professional. Highly recommended.

vibha R.
2 months ago
Heartfelt thanks to the entire team of Wellspring Hospital. After feeling disappointed and losing hope at many places, coming here was the best decision.
A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕
A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

Kanal G.
4 months ago
Some doctors treat symptoms. Rare ones treat the human being sitting in front of them.
He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.
He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Kul C.
6 months ago
Dr Shah is highly knowledgeable, through and dedicated. He explained every step of the process in simple terms, ensuring we were informed and comfortable. The entire team and staff are very kind and caring.
Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"
Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"

chandresh T.
6 months ago
We had a great experience with Wellspring. Dr Pranay Shah is a very good person and possess the good knowledge. His guidance and treatment helped us fulfill our wishes. The hospital staff is also very kind and supportive. I strongly recommend Wellspring.

Ruchita S.
8 months ago
I want to express my heartfelt gratitude to Dr. Pranay Shah and the team at Wellspring IVF & Women’s Hospital. This journey is never easy, but Dr. Shah made me feel comfortable, cared for, and fully supported throughout the IVF process. Thank you

Mohamed I.
8 months ago
Our hearts are overflowing with gratitude and joy as we reflect on our incredible journey to parenthood, made possible by the extraordinary care and expertise of your team. The IVF process was, at times, daunting and exhausting, but your unwavering support, compassion, and professionalism helped us remain hopeful through every step. From the very first consultation to the celebratory moment when we learned our treatment was successful, we felt respected, understood, and truly cared for.Thank you for believing in us, never giving up, and guiding us through every challenge with warmth, patience, and encouragement. Your personalized guidance, gentle approach, and positive outlook gave us strength, and your medical skill brought our dream to life. We are forever grateful for your remarkable ability to merge empathy and science, giving hope to couples like us.
Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Read all our verified Google reviews or share your own experience
Diagnosing Uterine Polyps — Dr. Shah's Approach
Dr. Pranay Shah follows a systematic, layered diagnostic approach that ensures no polyp — however small — is missed before an IVF cycle or fertility workup:
Step-by-Step Polyp Diagnosis at Wellspring IVF
Step-by-Step Polyp Diagnosis at Wellspring IVF
Step 1 — Transvaginal Ultrasound (TVS), Day 8–12
The proliferative phase (after menstruation, before ovulation) is when the endometrium is thinnest — making polyps most visible against the thin lining background. Dr. Shah specifically requests a mid-cycle TVS scan (day 8–12) rather than a generic ‘any time’ scan for maximum sensitivity. A hyperechoic (bright) endometrial focus with a regular margin and vascular stalk on Doppler is strongly suggestive of a polyp.
Step 2 — Saline Infusion Sonography (SIS)
When TVS is equivocal, or when a polyp is strongly suspected based on symptoms or history but TVS is non-diagnostic, SIS is performed. A small catheter is passed into the uterine cavity and sterile saline instilled — the fluid distends the cavity and makes any intracavitary lesion (polyp, septum, adhesion) immediately visible on ultrasound. Sensitivity for polyp detection approaches 95% with SIS. This is Dr. Shah’s preferred pre-IVF cavity assessment.
Step 3 — Diagnostic + Operative Hysteroscopy (See and Treat)
Hysteroscopy is both the gold-standard diagnostic tool AND the treatment — performed in the same sitting. Dr. Shah inserts a thin (3–5mm) hysteroscope through the cervix into the uterine cavity. Under direct camera vision, the entire cavity — fundus, both cornua, anterior and posterior walls — is systematically inspected. Any polyp identified is resected immediately using a hysteroscopic loop or grasper. No separate procedure. No second anaesthetic. One appointment, fully resolved.
Step 4 — Histopathology of Removed Tissue
All removed polyp tissue is sent for histological examination (biopsy analysis). This is not merely precautionary — it is mandatory. While the vast majority of premenopausal endometrial polyps are benign, histology provides definitive confirmation and detects the rare atypical hyperplasia or early malignancy. Results are reviewed with the patient at the follow-up consultation.
Step 5 — Post-polypectomy Cavity Confirmation
At the first menstrual cycle after polypectomy, Dr. Shah performs a follow-up TVS to confirm complete removal and normal cavity restoration before proceeding to IVF stimulation. If multiple polyps were present or the base was broad, SIS may be repeated to confirm a clean cavity.
Hysteroscopic Polypectomy — The Procedure, Step by Step
Operative hysteroscopy for polyp removal is one of the most straightforward, low-risk, high-reward procedures in reproductive medicine. Here is exactly what the procedure involves:
Setting & anaesthesia
Day-care procedure at Wellspring IVF. Performed under short general anaesthesia (15–30 minutes total). No overnight hospital admission required. The patient arrives fasted in the morning and is discharged home the same afternoon.
The approach — no incisions
A hysteroscope — a thin (3–5mm), rigid camera with a light source — is passed through the natural cervical opening into the uterine cavity. No cuts. No stitches. No abdominal incisions of any kind. The cervix is gently dilated if required (typically not necessary for a 3–5mm hysteroscope).
Visualisation & mapping
The uterine cavity is distended with sterile fluid (glycine or saline) to allow full visualisation. Dr. Shah systematically inspects the entire cavity — fundus, both cornua (tubal openings), anterior wall, posterior wall, and lower segment — before any resection. The polyp’s size, number, location, and attachment type (stalk vs broad base) are fully mapped.
Polypectomy technique
A prior pregnancy with Down Syndrome (Trisomy 21), Edwards Syndrome, Patau Syndrome, or other chromosomal conditions indicates elevated risk. PGT-A substantially reduces recurrence probability.
Procedure time
Single polyp: typically 10–15 minutes operative time. Multiple polyps: 20–30 minutes. Total procedure time including anaesthesia induction: 30–45 minutes.
After the procedure
Mild period-like cramping for 24–48 hours. Light spotting for up to 1 week. Normal activity typically resumed within 1–2 days. No heavy lifting or intercourse for 2 weeks. Oral antibiotics prescribed for 5 days to prevent infection.
When to proceed to IVF after polypectomy
IVF stimulation can commence after one full menstrual cycle following polypectomy — typically 4–8 weeks. This waiting period allows: complete healing of the endometrium at the polypectomy site, restoration of normal endometrial architecture, and receipt + review of histology results.
Success rate of polypectomy for improving IVF
Clinical pregnancy rates after hysteroscopic polypectomy and subsequent IVF are significantly higher than in untreated polyp patients. Multiple studies document a 50–100% improvement in implantation rates after complete polypectomy. The procedure consistently has one of the best cost-effectiveness ratios in reproductive medicine.
Found a Polyp on Scan? Don't Delay Your IVF Cycle — Clear It First.
Hysteroscopic polypectomy takes 30–45 minutes and can be scheduled within days. Your next IVF cycle can start just 4–6 weeks after.
Book Your Consultation
Call Us Now!
09099946050Polyps vs Fibroids vs Adenomyosis — Which Condition Do You Have?
Three conditions. Same organ. Overlapping symptoms. Completely different treatments. Here is how to distinguish them — and why getting the diagnosis right changes everything:
| Uterine Polyps | Fibroids / Adenomyosis | |
|---|---|---|
| What it is | Soft endometrial overgrowth — inside the cavity lining | Fibroids: muscular growths in/on uterine wall. Adenomyosis: lining in the muscle |
| Ultrasound appearance | Small, bright focus within endometrium. Clear margins | Fibroids: distinct round mass. Adenomyosis: bulky, heterogeneous wall |
| Can it be removed? | YES — completely, in a single hysteroscopy | Fibroids: myomectomy. Adenomyosis: cannot be removed — medical suppression only |
| Treatment time | 30–45 min day procedure. IVF in 4–8 weeks | Fibroids: surgery + 3–6 month recovery. Adenomyosis: 2–6 months GnRH suppression |
| Malignancy risk | Very low (0.3–3%). All tissue sent for histology | Fibroids: no malignancy risk. Adenomyosis: no malignancy risk |
| Recurrence | Can recur — particularly in oestrogen-dominant states | Fibroids: 10–15% at 5 years. Adenomyosis: returns after suppression stops |
Read our complete guides: Uterine Fibroids | Adenomyosis.
Symptoms of Uterine Polyps — From Obvious to Invisible
Polyps present across a spectrum — from women with severe bleeding to women with zero symptoms whose polyps are discovered only on pre-IVF hysteroscopy:
| Symptomatic Polyps | Silent Polyps — No Symptoms |
|---|---|
| Intermenstrual spotting (bleeding between periods) | Discovered only on pre-IVF SIS or hysteroscopy |
| Heavy menstrual bleeding (menorrhagia) | No bleeding abnormality at all |
| Irregular cycles — unpredictable periods | Normal ultrasound on 2D scan — missed due to cycle timing |
| Post-coital bleeding (after intercourse) | Recurrent IVF failure with 'unexplained' implantation failure |
| Post-menopausal bleeding — always investigate | Recurrent miscarriage with no other identified cause |
| Pelvic pressure or fullness (large polyps only) | Infertility — 'everything looks normal on your scan' |
Any bleeding after menopause requires urgent investigation. While polyps are a common cause, postmenopausal endometrial polyps carry a higher malignancy risk (up to 10–12% in some series) and must be removed and biopsied urgently. Do not attribute postmenopausal bleeding to polyps without confirmed histology.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah
Director & Chief Fertility Consultant

Divyesh Bhalodia
Senior Embryologist

Urmi Chauhan
Clinical Embryologist
Polyps, Recurrent Miscarriage & Unexplained Infertility
Two specific patient populations deserve particular attention — because in both, uterine polyps are a frequently missed treatable cause:
Recurrent Implantation Failure (RIF) After IVF
RIF is defined as failure to achieve pregnancy after transfer of 3 or more good-quality embryos. Before proceeding to a further IVF cycle, Dr. Shah performs a diagnostic hysteroscopy in all RIF cases — regardless of prior ultrasound findings.
In published series, intracavitary pathology — most commonly polyps — is found in 20–50% of RIF cases when hysteroscopy is performed, even when prior ultrasound scans were reported as normal. The polyp had been there, undetected, throughout the previous failed cycles.
Removing the polyp — and then proceeding to the next transfer — results in pregnancy in a significant proportion of RIF patients who had been told they simply ‘don’t respond to embryo transfer.’ The embryos were fine. The cavity was not.
Recurrent Miscarriage & Early Pregnancy Loss
Polyps at the implantation site interfere not just with initial attachment — they may also impair the early vascular invasion required for placentation. An embryo may implant ‘around’ the polyp but subsequently fail to develop normal placental blood flow, resulting in early miscarriage at 5–7 weeks.
In women with 2 or more unexplained miscarriages, hysteroscopy is now recommended as a routine investigation by the ESHRE (European Society of Human Reproduction and Embryology) Recurrent Pregnancy Loss guidelines. Intracavitary polyps found in this context should be removed before the next pregnancy attempt.
Before every IVF cycle at Wellspring IVF, I confirm the uterine cavity is clear. Not on a routine scan report from six months ago — on a fresh, properly timed assessment. In approximately 15–20% of women presenting for IVF, we find something in the cavity — most commonly a polyp. We remove it. The cycle is delayed by one month. And then we do the transfer into a clean, prepared cavity. That one month saves them two to three failed cycles — and the emotional and financial cost of those failures.
— Dr. Pranay Shah, MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
Frequently Asked Questions
Common questions about PGT-A, PGT-M, embryo biopsy, cost, and legal restrictions in India.
Ask a QuestionDo uterine polyps always need to be removed?
If the polyp is inside the uterine cavity and you are attempting pregnancy — either naturally or through IVF — yes, it should be removed. The evidence is clear that intracavitary polyps reduce IVF success rates and increase implantation failure risk. The procedure to remove it (hysteroscopic polypectomy) is simple, day-care, and low-risk. There is no rational argument for leaving a treatable physical barrier in place before a fertility treatment. For very small polyps (<5mm) found incidentally in women not actively trying to conceive, a watchful waiting approach with TVS follow-up may be appropriate — Dr. Shah discusses this individually.
How long after polypectomy before I can start IVF?
One full menstrual cycle — typically 4–8 weeks. This waiting period serves three purposes: it allows the endometrium to heal and regenerate at the polypectomy site; it provides time to receive and review the histology result; and it confirms, on a post-procedure scan, that the cavity is clear before starting stimulation. Attempting IVF stimulation in the immediate cycle after polypectomy is not recommended.
Can polyps come back after removal?
Yes. Polyps can recur — particularly in women with oestrogen-dominant states: PCOS, obesity, perimenopause, or those taking tamoxifen. The recurrence rate in the general population is approximately 15–20% within 5 years. Dr. Shah recommends annual TVS surveillance after polypectomy and specifically re-evaluates the cavity with SIS or hysteroscopy before each subsequent IVF cycle, regardless of how clear the previous scan was.
I had a 'normal' ultrasound scan — could I still have a polyp?
Yes — particularly if the scan was done at the wrong time of cycle, or if the polyp is small. A standard 2D TVS performed mid-cycle or late in the luteal phase (when the endometrium is thick) can miss polyps under 5–7mm. Dr. Shah performs TVS on day 8–12 of the cycle for maximum sensitivity. If clinical suspicion remains high — based on symptoms or failed IVF cycles — SIS or diagnostic hysteroscopy is arranged regardless of 2D TVS findings.
Is hysteroscopy painful? What is the recovery like?
Hysteroscopy for polypectomy at Wellspring IVF is performed under short general anaesthesia — the patient is completely asleep and experiences no discomfort during the procedure. After waking, mild period-like cramping is typical for 24–48 hours. Most women return to normal activity within 1–2 days. Light spotting for up to one week is normal. Sexual intercourse is avoided for 2 weeks post-procedure.
Can a polyp cause a miscarriage?
Yes. Intracavitary polyps are associated with both failed implantation and early pregnancy loss — through the mechanical and inflammatory mechanisms described above. In women with recurrent unexplained miscarriage, hysteroscopy is a recommended investigation. If a polyp is found, its removal before the next pregnancy attempt is strongly advisable — it is one of the most easily correctable causes of recurrent pregnancy loss.
Are uterine polyps cancerous?
The vast majority of endometrial polyps in premenopausal women are benign — non-cancerous. The malignancy risk is approximately 0.3–3% in reproductive-age women. This risk is higher in postmenopausal women (up to 10–12%). All polyp tissue removed during hysteroscopy at Wellspring IVF is routinely sent for histological analysis — providing definitive confirmation. Postmenopausal bleeding should always be investigated urgently, as the risk profile is different.
I've had two failed IVF cycles. Should I have a hysteroscopy before trying again?
Yes — this is strongly recommended. Recurrent implantation failure (2+ failed transfers with good embryos) is a clear indication for diagnostic hysteroscopy — regardless of what prior ultrasound scans have shown. In published series, intracavitary pathology (most commonly polyps) is found in 20–50% of RIF cases when hysteroscopy is performed after normal ultrasound. At Wellspring IVF, hysteroscopy is a standard investigation before any third IVF cycle.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026

Complete Information Map
Related Conditions & Treatments
Female Infertility Hub — All Female Causes
Hysteroscopy at Wellspring IVF — Full Procedure Guide
Uterine Fibroids — Location Matters More Than Size
A Polyp Is the Most Fixable Cause of IVF Failure.
One 30-minute procedure. No incisions. Home the same day.
If you have a polyp on your scan, a history of failed implantation, or abnormal bleeding — do not delay. Dr. Pranay Shah will confirm the diagnosis, remove the polyp, and get your uterine cavity IVF-ready.
If you have a polyp on your scan, a history of failed implantation, or abnormal bleeding — do not delay. Dr. Pranay Shah will confirm the diagnosis, remove the polyp, and get your uterine cavity IVF-ready.