Normal Zona Pellucida
Thin, elastic shell
The embryo expands naturally, applying internal pressure. The zona thins and ruptures spontaneously. Embryo hatches and implants.
No LAH needed
Precision Infrared Laser | Contactless Procedure | Targeted for Specific Clinical Groups
Every embryo, before it can attach to the uterine wall and begin a pregnancy, must first break free of its protective outer shell — the zona pellucida. In most IVF cycles, this hatching happens naturally. In some patients, the zona is too thick or too hardened for the embryo to rupture it on its own — and the cycle fails despite a perfectly healthy embryo inside.
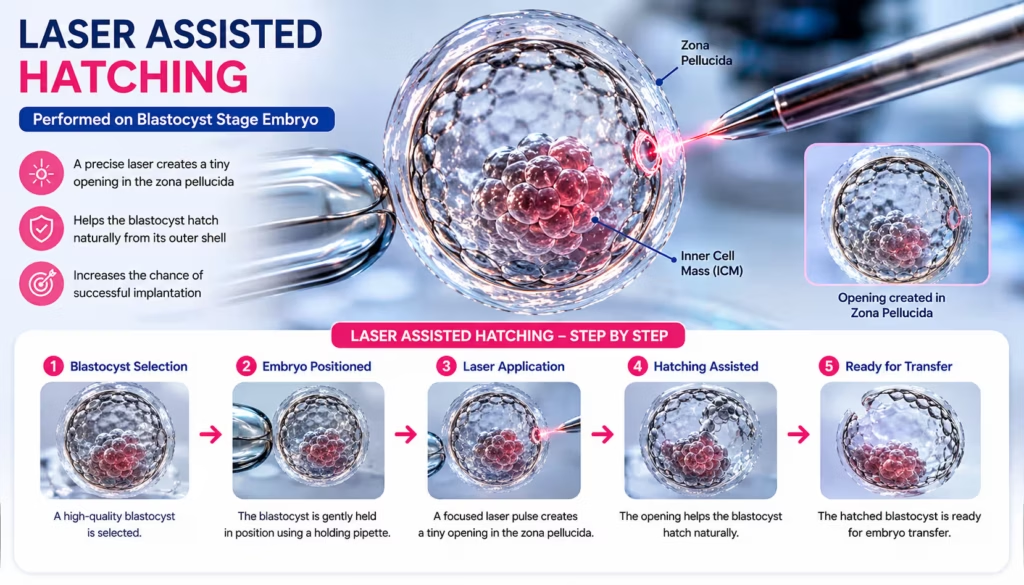
Laser Assisted Hatching (LAH) is the solution to that specific problem. Wellspring IVF’s embryologists use a precision infrared laser to create a microscopic opening in the zona pellucida — a procedure that takes less than one second, never contacts the embryo directly, and is performed immediately before embryo transfer. It is not a treatment we offer to every patient. It is a precisely targeted intervention for those who genuinely need it.
Think of the zona pellucida as an eggshell made of protein — flexible in young, healthy eggs, but capable of becoming rigid under certain conditions. This shell has two jobs: protect the embryo during its early divisions, then break open (hatch) at Day 5–6 so the embryo can emerge and attach to the uterine lining.
When the shell is too thick — whether due to maternal age, cryopreservation, or other factors — the embryo cannot generate enough internal pressure to break through. It is physically trapped inside a shell it cannot escape. The implantation window closes. The cycle fails. This is not a failure of the embryo’s developmental potential — it is a mechanical barrier.
The laser does not touch the embryo. It targets only the zona itself — creating an opening of approximately 15–20 microns, which is 1/5th the width of a human hair.
As women age, the zona pellucida naturally becomes thicker and less elastic. This is a well-documented biological change that occurs in parallel with the broader decline in egg quality associated with age. Even when an older egg produces a viable, developmentally competent embryo, the zona may be too rigid for that embryo to hatch without assistance.
Published data shows that assisted hatching provides a measurable benefit in women over 37 undergoing IVF — particularly for those using their own eggs. Dr. Shah assesses zona thickness under the microscope before every transfer in this age group and makes a case-by-case decision.
Dr. Shah’s clinical threshold: Zona pellucida thickness >15 microns on microscopic assessment is a primary indicator for LAH recommendation, regardless of embryo grade.
Cryopreservation — the process of freezing embryos using Vitrification — is one of the most significant advances in IVF. However, the freezing and thawing process can cause changes in the zona pellucida that make it harder and less elastic than it was before freezing. This is not a flaw in the Vitrification process — it is a known biological response to the cryoprotectant chemicals used during freezing.
For patients undergoing a Frozen Embryo Transfer (FET) — particularly with older frozen embryos or embryos from patients over 35 — Dr. Shah routinely evaluates whether the zona has hardened post-thaw and applies LAH when indicated. The laser is performed on the thawed embryo before transfer, typically within 2–4 hours of thaw completion.
Key fact: The thawed embryo is assessed under high-magnification microscopy to measure zona thickness before every FET. LAH is not automatically applied to every frozen transfer — only those where post-thaw zona hardening is observed or clinically suspected.
When a couple has undergone two or more IVF cycles with good-quality embryos and no pregnancy, the word ‘unexplained’ carries enormous emotional weight. Dr. Shah’s approach to recurrent implantation failure (RIF) is systematic: rule out every identifiable cause before concluding that nothing can be improved.
Zona pellucida thickness is one of several factors evaluated in the RIF workup. If it is found to be abnormal — or if other causes have been excluded and LAH has not yet been tried — it becomes part of the therapeutic escalation. In this context, LAH is one tool within a broader recurrent failure protocol that may also include:
LAH in RIF patients is not prescribed in isolation — it is part of a reasoned, investigative protocol. Patients who have had multiple failures deserve a systematic explanation, not just another cycle with a new add-on.
Dr. Pranay Shah explicitly does not recommend LAH as a routine addition to every IVF cycle. The evidence does not support universal LAH for all IVF patients — and applying it indiscriminately does not improve outcomes in low-risk groups. At Wellspring, LAH is never offered as a ‘premium upgrade.’ If you are in this group, you will be told clearly:
If you have been told you need LAH at another clinic without any of the above indications — or without a clear explanation of why — we encourage you to ask for the clinical rationale. Wellspring’s position: unnecessary LAH is not risk-free and not evidence-based for unselected patients. We will never charge for a procedure you don’t need.
Learn how Laser Assisted Hatching works, how it safely enhances embryo implantation success during IVF, and exactly which clinical groups benefit from it according to Dr. Pranay Shah.
The Role of the Zona Pellucida: Understand the protein “eggshell” surrounding the embryo and why it must naturally thin out and rupture before successful implantation can take place.
How the Precision Laser Works: Discover how our embryologists use a contactless infrared laser to create a microscopic 15–20 micron opening in milliseconds, without ever touching the inner cells of the embryo.
Dr. Shah’s 3 Clear Target Groups: Learn why LAH is not a marketing upgrade for everyone, but a vital clinical tool specifically indicated for women aged 35+, Frozen Embryo Transfers (FET), and Recurrent IVF Failures.
Debunking 4 Common LAH Myths: Find out the scientific truths regarding embryo safety, identical twinning risks, and why it is used as a highly personalized supportive technique rather than a blanket guarantee.
The procedure itself is performed entirely within our IVF laboratory, by our senior embryologist, on the morning of embryo transfer. Here is exactly what happens:
| Step | What Happens | Duration |
|---|---|---|
| 1. Embryo Assessment Under Microscope | The embryo selected for transfer is placed under high-magnification microscopy. The embryologist measures zona pellucida thickness at multiple points. Zone hardening post-thaw is visually assessed. | 5–10 minutes |
| 2. Embryo Positioned in Holding Dish | The embryo is stabilised in a specialised holding medium within a microscopy dish. Temperature maintained at 37°C throughout to prevent any cold shock. | 2–3 minutes |
| 3. Infrared Laser Targeting | The embryologist uses a computer-controlled infrared laser (1480nm wavelength — the most commonly used standard) to target a precise point on the zona pellucida. The laser beam is focused to a diameter of approximately 15–20 microns. | < 30 seconds |
| 4. Single Laser Pulse | One brief laser pulse (typically 1–5 milliseconds) ablates a small channel through the zona. The laser never touches the embryo’s cells — only the zona shell. The embryo remains completely protected inside. | < 1 second |
| 5. Visual Verification | The embryologist immediately confirms under the microscope that the opening is present and correctly sized. No over-ablation or embryo damage is verified before proceeding. | 2–5 minutes |
| 6. Embryo Transferred | The embryo is loaded into the transfer catheter and transferred to the uterus by Dr. Pranay Shah within 1–2 hours. Standard transfer protocol proceeds. | 20–30 minutes |
“The precision of the infrared laser we use is extraordinary. The entire zona opening takes less time than a single heartbeat. What impresses patients most when I explain it is that the laser never once touches the embryo — it operates exclusively on the protein shell. We are not altering the embryo in any way. We are simply removing a physical barrier that was standing between that embryo and its ability to implant.”
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.



Understanding when LAH helps — and when it doesn’t — is the core of Dr. Shah’s selective approach. This table summarises the key clinical distinctions:
| Factor | Without LAH | With LAH (Targeted Cases) |
|---|---|---|
| Who it applies to | Young patients, normal ZP, standard IVF | Advanced age 35+, FET cycles, thick ZP, recurrent failure |
| ZP thickness | Normal (thin, elastic) | Thick or hardened (cryopreservation effect) |
| Hatching mechanism | Natural — embryo ruptures ZP spontaneously | Assisted — laser creates a precise opening before transfer |
| Implantation window risk | Low — natural hatching synchronised | High without LAH — thick ZP may trap embryo in the window |
| Laser involved? | No | Yes — infrared, contactless, <1 second exposure |
| Embryo contact? | N/A | None — laser targets only the zona, never the embryo cells |
| Expected benefit? | No additional benefit for standard patients | Published data: 10–25% relative improvement in implantation for target groups |







The published evidence on LAH is consistent in one key finding: benefit is highly patient-group specific. The same systematic reviews that show significant improvement in targeted groups show no meaningful benefit in unselected young IVF patients. Here is the honest evidence summary:
| Patient Group | LAH Benefit on Implantation Rate | Evidence Quality | Dr. Shah’s Recommendation |
|---|---|---|---|
| Women 37+ using own eggs | 10–20% relative improvement in implantation | Moderate — multiple RCTs | Recommended — assess zona before each transfer |
| FET cycles (all ages) | 8–18% relative improvement post-thaw zona hardening | Moderate — consistent across FET studies | Recommended — evaluate every thawed embryo |
| Recurrent implantation failure (2+ failed cycles) | Variable — 10–25% relative improvement in some studies | Moderate — part of systematic escalation | Recommended as part of RIF protocol |
| Young women (<35), first IVF, normal zona | No statistically significant benefit in meta-analyses | High — Cochrane review | Not recommended — evidence does not support routine use |
| All IVF patients regardless of indication | Marginal, inconsistent across studies | Mixed quality | Not recommended — Wellspring does not offer universal LAH |
The most comprehensive systematic review of assisted hatching (Cochrane Database, updated 2021) concluded: ‘There is moderate-quality evidence that assisted hatching improves live birth rates in poor-prognosis patients — specifically those with failed previous cycles and those with frozen embryos. The evidence does not support routine assisted hatching for all IVF/ICSI patients.’ Wellspring’s selective approach is directly aligned with this conclusion.
Patient anxiety about laser use near embryos is completely understandable — and completely addressable with the facts. Here is the complete safety profile of the infrared laser used in LAH at Wellspring:
Wavelength: 1480nm infrared (non-ionising, thermal effect only)
Mechanism: Thermal ablation of zona protein — water in the zona absorbs the infrared energy and vaporises the protein locally
Target zone: Zona pellucida only — the laser is focused on the shell, not the embryo
Pulse duration: 1–5 milliseconds (one thousandth of a second)
Opening size: 15–20 microns (1/5th the width of a human hair)
Embryo contact: None — the laser operates exclusively on the zona
Laser Assisted Hatching has been in clinical use since 1989. Over 35 years of outcome data — across hundreds of thousands of IVF cycles worldwide — shows no safety signal against its use in indicated patients.
Yes — always. The decision to perform LAH is discussed with the patient before the transfer day during the embryo transfer planning consultation. If Dr. Shah recommends LAH based on your age, transfer type (FET), or history, he will explain the clinical rationale clearly. LAH is never applied without your knowledge and consent. On the day of transfer, if the thawed embryo’s zona assessment reveals unexpected hardening, the embryologist will contact you before proceeding.
No. The procedure is performed on the embryo in the laboratory — not on you. You will not feel anything. The embryo transfer procedure that follows is the same as a standard transfer: a thin catheter is guided through the cervix to the uterus under ultrasound guidance. Most patients describe the transfer as feeling similar to a Pap smear. No sedation is required. You go home the same day.
At Wellspring, LAH is performed on Day 5 blastocysts — not Day 3 cleavage stage embryos. The blastocyst stage is preferred because the embryo has already demonstrated its developmental capacity, the zona is thinner at this stage (making precise laser targeting more straightforward), and the trophectoderm (outer cell layer) is well-developed and resilient. For FET cycles, LAH is performed on the morning of transfer, after the embryo has been thawed and assessed. Read more about our Blastocyst Culture protocol at Wellspring.
Laser Assisted Hatching is not a standalone charged procedure at Wellspring when it is clinically recommended as part of your IVF or FET cycle — it is included in the comprehensive cycle cost when indicated. At your initial consultation or FET planning appointment, Dr. Shah will provide a complete itemised cost breakdown that reflects your individual treatment plan. Call 9099946050 for current pricing information.
You can ask about it — and Dr. Shah will always explain his reasoning. However, Wellspring’s position is clear: if the clinical indication for LAH is not present, recommending it would not be evidence-based and would not be in the patient’s interest. An honest ‘no’ from Dr. Shah — with a clear explanation of why your specific situation does not require it — is a mark of the ethical, personalised care philosophy at Wellspring. We do not perform procedures because a patient requests them if the evidence does not support benefit for their specific clinical profile.
Recurrent implantation failure is a complex clinical challenge — and LAH is one part of a broader investigative protocol, not a standalone solution. Before recommending LAH for a recurrent failure patient, Dr. Shah will systematically review: embryo quality across all cycles, zona thickness measurements from previous cycles, uterine cavity condition (hysteroscopy), endometrial receptivity (ERA test if indicated), genetic factors (PGT-A on embryos), and immune/clotting factors. LAH may form part of the next cycle plan — but only as one element within a reasoned protocol designed specifically for your situation. Please go through our Recurrent Miscarriage page for the full workup framework.
Clinical studies show a very slight, marginal increase in the rate of identical (monozygotic) twinning when any form of micro-manipulation—including Laser Assisted Hatching or ICSI—is performed on an embryo’s shell. However, the absolute baseline risk remains extremely low (around 1–2%). Dr. Pranay Shah and our embryology team use an ultra-precise, micro-targeted laser pulse that creates only a minimal, clean opening (15–20 microns) without altering the inner cell mass, ensuring the structural integrity of the embryo is maintained while safely facilitating natural implantation.