Recurrent Miscarriage Treatment in Ahmedabad— Finding the Why Before Trying Again
After the second: "These things happen. Try again."
After the third, you stopped accepting that answer. And you were right not to.
Recurrent miscarriage — defined clinically as two or more consecutive pregnancy losses — affects 1–2% of couples. It is not just bad luck. After multiple losses, there is a 40–50% probability of an identifiable, specific, treatable cause — if the right investigations are performed by a clinician who knows what to look for.
At Wellspring IVF & Women's Hospital, Dr. Pranay Shah approaches recurrent pregnancy loss as a clinical detective — not a statistician. His approach is not to reassure you with probabilities. His approach is to investigate systematically, identify the specific cause in your case, and treat it with precision — so that the next pregnancy is not another attempt at hope, but a medically informed, strategically prepared success.
The Most Important Reframe on This Page
‘Try again’ is not a treatment plan.
Investigation is a treatment plan. In RPL, finding the cause IS the first treatment — because you cannot fix what you have not identified.
Dr. Shah’s RPL workup identifies the specific cause in approximately 50–60% of couples who had previously been told ‘everything is normal.’
Recurrent Miscarriage — At a Glance
Recurrent miscarriage is one of the most emotionally devastating experiences in medicine. The grief of each loss is real, valid, and deserving of proper acknowledgement — not statistics.
“This page is written for couples who are ready — when they are ready — to understand why this has happened and what can be done. There is no pressure to act immediately. There is only the commitment that Dr. Pranay Shah will find the answer — and treat it.”
 Recurrent Miscarriage — At a Glance
Recurrent Miscarriage — At a Glance 9099946050
9099946050What Is Recurrent Miscarriage? — Understanding RPL
Recurrent Pregnancy Loss (RPL) is defined by most international guidelines (ESHRE, ASRM) as two or more pregnancy losses — including biochemical pregnancies (positive blood test, no ultrasound confirmation), early losses before 6 weeks, and losses after a confirmed heartbeat.
The distinction matters because the emotional weight of each loss is identical — whether it was a faint positive test that disappeared at 4 weeks, or a loss at 8 weeks after seeing a heartbeat. All of these count. All deserve investigation.
Two critical numbers for context: approximately 15–20% of all clinically recognised pregnancies end in miscarriage — so in any group of women, some will experience two losses by statistical chance alone. But once you reach a third loss, the probability that chance alone explains this drops to under 1%. There is almost certainly an underlying cause.
The Recurrent Implantation Failure (RIF) Connection:
Many couples who experience RPL also have a history of IVF cycles where embryos failed to implant — or implanted briefly and then were lost. Recurrent implantation failure (RIF) and recurrent miscarriage share several root causes — particularly chromosomal abnormalities, thrombophilia, and uterine cavity pathology. Dr. Shah investigates both simultaneously with the same workup.
The 4 Core Causes of Recurrent Miscarriage — Dr. Shah's Investigation Framework
Every couple presenting with RPL at Wellspring IVF undergoes a structured, systematic workup across four domains. Here is what is looked for in each — and exactly how each is treated when found:
Genetic / Chromosomal — The #1 Cause
Responsible for 50–60% of individual miscarriages and 30–40% of RPL cases
What happens: During fertilisation, errors can occur in how chromosomes are divided between cells. An embryo with an abnormal number of chromosomes (aneuploidy) — too many or too few — cannot develop into a viable pregnancy. The body recognises this and expels the pregnancy, typically before 10 weeks. This is not a failure of the mother’s body. It is the body working correctly — rejecting an embryo that cannot survive. The tragedy is that it looks and feels like a miscarriage.
Why it causes RPL: Aneuploidy rate increases with maternal age — rapidly after 35 and dramatically after 38. However, some younger women have eggs with inherently higher error rates due to ovarian reserve issues, genetic conditions, or paternal sperm DNA fragmentation. If the underlying egg or sperm quality issue is not addressed, each new embryo carries the same chromosomal risk.
Investigation — Parental Karyotyping: Blood test for both partners. Identifies rare but important structural chromosomal abnormalities (translocations, inversions) that consistently produce unbalanced embryos. Found in approximately 2–5% of RPL couples — but critical when present because it changes the entire treatment strategy.
Investigation — Products of Conception (POC) Genetic Testing: When a miscarriage occurs, Dr. Shah requests that the products of conception (when accessible) are sent for chromosomal analysis — FISH or microarray. If the lost pregnancy was chromosomally abnormal, this is direct evidence that aneuploidy was the cause. This result transforms the next treatment decision.
The Solution — PGT-A (Preimplantation Genetic Testing for Aneuploidies): IVF with PGT-A is the single most powerful intervention for chromosomally-driven RPL. Embryos are created via IVF, cultured to blastocyst stage (day 5), biopsied for genetic analysis, and only chromosomally NORMAL (euploid) embryos are transferred. The miscarriage rate after PGT-A transfer of a euploid embryo drops to approximately 5–10% — compared to 20–40% in unscreened transfers. For a couple who has lost 3 or 4 pregnancies, transferring a confirmed-normal embryo changes the clinical picture entirely.
Sperm DNA Fragmentation: Often overlooked in RPL investigation. High levels of sperm DNA damage produce embryos that fertilise normally but carry hidden genetic damage that causes early arrest or miscarriage after initial implantation. Dr. Shah includes DFI (DNA Fragmentation Index) testing in all RPL workups — particularly when previous losses occurred after a heartbeat was confirmed.
Anatomical — Physical Barriers in the Uterine Cavity
Found in approximately 10–15% of RPL couples — often completely reversible with surgery
Uterine Septum — The Most Common Structural Cause: A uterine septum is a band of avascular (non-blood-supply) fibrous tissue that divides the uterine cavity. An embryo that implants on the septum cannot establish normal placentation — because the septum has no blood supply. The pregnancy implants, a heartbeat may develop, and then at 8–12 weeks the blood supply fails and the pregnancy is lost. This pattern — loss after a confirmed heartbeat — is strongly suggestive of a septal or vascular anatomical cause. Diagnosed by 3D TVS or hysteroscopy. Treatment: hysteroscopic metroplasty (septum incision) — day procedure, no incisions.
Uterine Polyps and Submucosal Fibroids: Both cause mechanical interference with implantation and placentation. A polyp or submucosal fibroid at the implantation site creates an abnormal blood supply environment — the embryo may implant but cannot develop normal placental vascular connections. Both are treated by hysteroscopic removal — the same day-care procedure.
Intrauterine Adhesions (Asherman’s Syndrome): Scarring within the uterine cavity — most commonly caused by prior D&C procedures (including previous miscarriage management), infection, or surgery. Adhesions physically block the cavity and reduce endometrial blood flow. Diagnosed on hysteroscopy. Treated by hysteroscopic adhesiolysis.
Arcuate Uterus vs Bicornuate Uterus: Minor uterine shape variants (arcuate uterus) are likely not clinically significant for miscarriage. Major variants (bicornuate, unicornuate, didelphys) are associated with RPL. Diagnosed on 3D TVS or MRI. Management depends on severity — most do not require surgical intervention.
Investigation and Treatment: All anatomical causes are assessed by: 3D TVS + SIS (saline infusion sonography) + diagnostic/operative hysteroscopy. Where hysteroscopy identifies a correctable lesion — septum, polyp, fibroid, adhesions — operative removal is performed in the same sitting.
Immunological / Clotting — The Silent Thrombus
Antiphospholipid Syndrome found in 15–20% of RPL cases — fully treatable
Antiphospholipid Syndrome (APS) — The Critical Diagnosis: APS is an autoimmune condition in which the body produces antibodies (anticardiolipin, anti-beta-2 glycoprotein, lupus anticoagulant) that trigger microscopic clotting within the placental blood vessels. The placenta normally forms a rich vascular network during weeks 8–12 — this is precisely when APS-related placental thrombosis occurs, causing sudden loss of blood supply to the developing pregnancy. The miscarriage occurs at 8–14 weeks, typically after a confirmed heartbeat. APS is found in 15–20% of women with RPL and is one of the most important treatable causes of late first-trimester and second-trimester pregnancy loss.
Other Inherited Thrombophilias: Factor V Leiden mutation, Prothrombin gene mutation, MTHFR variants, Protein C and Protein S deficiency — these inherited clotting tendencies impair placental microvascular development at critical stages. Their contribution to RPL is debated in the literature — Dr. Shah interprets results in clinical context, not in isolation.
Investigation — Thrombophilia Screen: Full panel: anticardiolipin antibodies (IgG and IgM), anti-beta-2 glycoprotein antibodies, lupus anticoagulant — tested twice, 12 weeks apart (APS requires two positive tests to confirm). Plus: Factor V Leiden PCR, Prothrombin gene, Protein C, Protein S, MTHFR mutation testing.
NK Cell Testing — A Note on Controversy: Elevated natural killer (NK) cells in the endometrium have been proposed as a cause of RPL in some clinics — and expensive immunological treatments offered on this basis. Dr. Shah’s approach: the evidence for NK cell testing and treatment in RPL remains inconclusive per current ESHRE guidelines. He does not recommend or offer this testing routinely — patients deserve evidence-based clarity, not expensive tests of uncertain value.
The Treatment — LMWH + Low-Dose Aspirin Protocol: Confirmed APS or significant thrombophilia is treated with: Low Molecular Weight Heparin (LMWH — Clexane/Enoxaparin) — a subcutaneous injection started with a positive pregnancy test and continued through 34 weeks gestation, plus low-dose aspirin (75–100mg) started pre-conception. With this protocol, live birth rates in APS patients improve from approximately 10% (untreated) to 70–80%. This is one of the most dramatic treatment success stories in reproductive medicine.
Hormonal / Endocrine — The Invisible Imbalance
Thyroid, progesterone, insulin — all measurable, all correctable
Thyroid Dysfunction — The Most Commonly Missed Hormonal Cause: Subclinical hypothyroidism — a mildly elevated TSH (2.5–4.5 mIU/L) with normal T3/T4 — is associated with a 2–3 fold increase in miscarriage risk and is found in a significant proportion of RPL patients. Overt hypothyroidism (TSH >4.5) and Hashimoto’s thyroiditis (positive anti-TPO antibodies) carry even higher risk. The key: standard ‘normal’ thyroid range is too broad for pregnancy — Dr. Shah targets TSH <2.5 mIU/L in all fertility patients and treats subclinical hypothyroidism with low-dose levothyroxine before attempting conception.
Progesterone Deficiency — The Luteal Phase Problem: Progesterone is the hormone that maintains the uterine lining after ovulation and supports implantation and early placentation. Inadequate progesterone levels — luteal phase defect — can result in early pregnancy loss before the placenta takes over progesterone production at 10–12 weeks (the luteal-placental shift). Diagnosed by mid-luteal progesterone levels or progesterone levels in early pregnancy. Treated with progesterone supplementation (vaginal pessaries/gel or intramuscular injection) from positive pregnancy test through 12–16 weeks.
Insulin Resistance and PCOS: Women with PCOS and insulin resistance have elevated LH levels, androgens, and abnormal glucose metabolism — all of which impair embryo quality and endometrial receptivity. Metformin therapy in insulin-resistant women with PCOS has been shown in multiple studies to reduce miscarriage rates in both natural and IVF cycles.
Poorly Controlled Diabetes: Maternal hyperglycaemia (high blood sugar) in early pregnancy is associated with significantly elevated miscarriage rates and congenital abnormalities. Pre-conception HbA1c target: <6.5% (48 mmol/mol). Dr. Shah requests fasting glucose and HbA1c in all RPL workups, particularly in women with PCOS, obesity, or family history of diabetes.
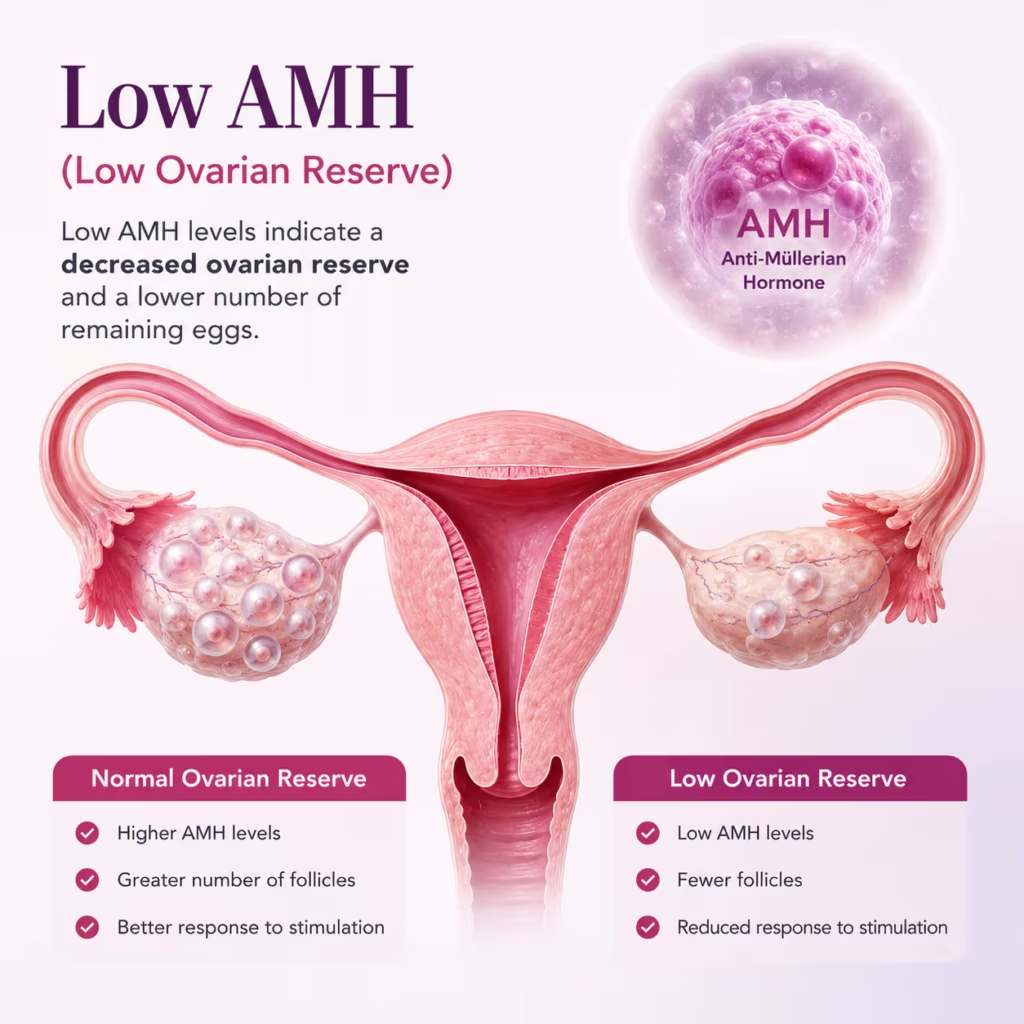
Investigation — Hormonal Panel for RPL: TSH + Anti-TPO antibodies. Fasting glucose + HbA1c. AMH + Day 3 FSH/LH + oestradiol (ovarian reserve). Mid-luteal progesterone (Day 21 of natural cycle or equivalent). Prolactin. All tests available as a single coordinated panel.
PGT-A — The Game-Changing Tool for Recurrent Miscarriage
For couples whose RPL investigation identifies — or strongly suggests — chromosomal causes, PGT-A (Preimplantation Genetic Testing for Aneuploidies) is the single most clinically significant tool in modern reproductive medicine.
PGT-A answers a question that no other test can answer: “Is this embryo chromosomally normal?” — before it is transferred. Before a pregnancy is established. Before another loss occurs.
PGT-A — Complete Guide for RPL Patients
What PGT-A tests
PGT-A screens all 24 chromosomes (22 autosomes + X and Y) in each embryo for numerical abnormalities — extra or missing chromosomes (trisomy, monosomy). An embryo with the correct number of chromosomes in every cell is called euploid. Only euploid embryos are transferred. An aneuploid embryo — one with chromosomal abnormalities — is not transferred. It would have resulted in miscarriage or implantation failure.
How the test works
IVF stimulation → egg retrieval → fertilisation with ICSI → embryo culture to blastocyst stage (Day 5) → trophectoderm biopsy (a few cells removed from the outer layer of the blastocyst — the future placenta, not the embryo itself) → cells sent to genetics laboratory → NGS (Next Generation Sequencing) analysis → embryo frozen while results are awaited (typically 7–14 days) → only euploid embryos thawed and transferred in FET cycle.
Success rates with PGT-A in RPL
In RPL patients, the live birth rate per euploid embryo transfer is approximately 60–70% — compared to 30–40% for unscreened transfers. More critically, the miscarriage rate after confirmed-euploid transfer drops to 5–10% — regardless of maternal age. For a woman who has lost 3 pregnancies, transferring a genetically confirmed normal embryo fundamentally changes the odds.
Who benefits most from PGT-A
Advanced maternal age (>35): aneuploidy rate rises steeply. 3+ miscarriages with no other identifiable cause. Previous miscarriage with confirmed chromosomal abnormality on POC testing. Recurrent implantation failure after IVF with good embryos. High sperm DNA fragmentation (>25% DFI) affecting embryo chromosomal integrity.
An important nuance — mosaic embryos
PGT-A occasionally identifies ‘mosaic’ embryos — those with a mix of normal and abnormal cells. Current evidence suggests some mosaic embryos can develop into healthy pregnancies. Dr. Shah discusses mosaic embryo transfer individually with each couple, with full transparency about the available evidence and the specific chromosomal finding.
Is PGT-A right for everyone with RPL
Not necessarily. If RPL is caused by APS (immunological) or anatomical factors that have been treated, PGT-A adds cost without necessarily improving outcomes further. Dr. Shah recommends PGT-A selectively — based on the RPL workup results, maternal age, number of prior losses, and prior IVF history. The recommendation is always individualised and fully explained.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
The Wellspring IVF RPL Investigation Panel — Complete Workup
Every couple presenting with recurrent pregnancy loss undergoes a coordinated, simultaneous investigation across all four cause domains. Here is the complete workup — both partners investigated from Day 1:
| Test / Investigation | What It Identifies | Positive Result | Both/Which Partner |
|---|---|---|---|
| Parental karyotype (both) | Chromosomal translocations / structural abnormality | Referral to genetic counsellor + PGT-A | Both partners |
| Sperm DNA Fragmentation (DFI) | Paternal DNA damage contributing to embryo loss | Antioxidant therapy + consider ICSI/IMSI | Male partner |
| POC genetic testing (if accessible) | Confirms if loss was chromosomally driven | Confirms need for PGT-A | Products of conception |
| 3D TVS + SIS | Uterine septum, polyps, fibroids, adhesions | Operative hysteroscopy planned | Female partner |
| Diagnostic Hysteroscopy | Definitive cavity assessment + treat-in-same-sitting | Polypectomy / metroplasty / adhesiolysis | Female partner |
| Antiphospholipid antibodies (×2, 12 wks apart) | APS — primary immunological cause of RPL | LMWH + aspirin protocol commenced | Female partner |
| Thrombophilia screen (Factor V, Prothrombin, Protein C/S) | Inherited clotting disorders | Individualised anticoagulation plan | Female partner |
| TSH + Anti-TPO antibodies | Thyroid dysfunction / Hashimoto’s | Levothyroxine — target TSH <2.5 | Female partner |
| Fasting glucose + HbA1c | Diabetes / insulin resistance | Metformin / glycaemic optimisation | Female partner |
| AMH + Day 3 FSH/LH/E2 | Ovarian reserve — informs PGT-A decision | Counselling on egg quality + PGT-A | Female partner |
| Mid-luteal progesterone | Luteal phase defect | Progesterone supplementation protocol | Female partner |
| Prolactin | Hyperprolactinaemia — disrupts luteal phase | Cabergoline / bromocriptine | Female partner |
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Treatment After RPL Investigation — Dr. Shah's Protocol
Chromosomal / Genetic — IVF with PGT-A
Stimulation → blastocyst culture → trophectoderm biopsy → NGS analysis → freeze-all → euploid FET. For paternal DNA fragmentation: antioxidant therapy (CoQ10, Vitamin C/E, zinc) for 90 days + ICSI or IMSI technique. For parental translocation: PGT-SR (Structural Rearrangement) added to PGT-A.
Anatomical — Operative Hysteroscopy
Septum: hysteroscopic metroplasty — incise the septum under camera vision. Polyps: hysteroscopic polypectomy — full guide at Uterine Polyps page. Fibroids (submucosal): hysteroscopic resection. Adhesions: hysteroscopic adhesiolysis + postoperative oestrogen support. After anatomical correction: spontaneous conception or IUI attempted first; IVF if not successful within 3–6 cycles.
Immunological / Clotting — LMWH + Aspirin Protocol
Confirmed APS: LMWH (Clexane 40mg) daily SC injection from positive pregnancy test, continued through 34 weeks. Low-dose aspirin (75mg) daily from pre-conception. Monitor platelet count and anti-Xa levels. For Factor V Leiden homozygous: higher dose LMWH + haematology co-management. Expected outcome: live birth rate improvement from ~10% to 70–80%.
Hormonal / Endocrine — Targeted Correction
Hypothyroidism: levothyroxine titrated to TSH <2.5 before conception attempt. Progesterone deficiency: micronised progesterone 200–400mg vaginally twice daily from positive test through 12–16 weeks. PCOS/insulin resistance: metformin + lifestyle + ovulation induction as appropriate. Hyperprolactinaemia: cabergoline to normalise prolactin before conception.
When No Cause Is Found — Unexplained RPL
In 40–50% of RPL cases, the full workup returns normal. This is not a failure of investigation — it is the current limit of medical science. Management in unexplained RPL includes: empirical progesterone supplementation (low risk, possible benefit), folic acid + aspirin + supportive care. For unexplained RPL after 3+ losses, PGT-A-assisted IVF is offered — even without identified genetic cause — as it reduces the aneuploidy risk that may not have been detected on parental karyotype. Regular early ultrasound surveillance in subsequent pregnancy for reassurance and early detection of problems.
💬 Had 2 or More Miscarriages? You Deserve a Real Answer.
What to Expect in Your Next Pregnancy After RPL Treatment
One of the most important conversations at Wellspring IVF is managing the anxiety of a subsequent pregnancy after recurrent losses. A positive test no longer feels like joy — it feels like waiting for loss. This is normal, valid, and does not reflect weakness.
Dr. Shah’s Subsequent Pregnancy Monitoring Protocol
Week 5–6: First transvaginal scan — confirm intrauterine location and early sac.
Week 6–7: Second scan — confirm fetal pole and cardiac activity.
Week 8: Third scan — confirm ongoing heartbeat and growth. APS/thrombophilia patients: LMWH dose and compliance reviewed.
Week 10–12: Combined first trimester screening (NIPT + NT scan). Progesterone supplementation reviewed and weaned where appropriate.
Throughout: Additional early scans available for reassurance at any point. Dr. Shah is accessible by WhatsApp for interim concerns between scheduled appointments — because a two-week wait after a previous loss is not clinically acceptable.
“When a couple sits in front of me after a third miscarriage, the last thing they need is another reassuring statistic. They need someone to look at their complete history — all of it — and say: this is what is happening in your specific case, and this is what we are going to do about it. In my experience, if you look properly, you find the answer in the majority of cases. And in the cases where the tests come back normal — we have PGT-A to remove the chromosomal variable entirely. There is always a next step. There is always something we can do better than the previous cycle.”
— Dr. Pranay Shah, MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
How many miscarriages before I should seek specialist evaluation?
Formally, ESHRE and ASRM define RPL as two or more losses — and investigation is recommended after two. However, many guidelines acknowledge that investigation after a second loss is clinically justified, particularly in women over 35 where time is a factor. Dr. Shah will perform a basic RPL screen after two losses without requiring a third. Earlier investigation is always reasonable if you choose not to wait.
Is miscarriage always caused by a genetic problem?
Genetic (chromosomal) abnormalities in the embryo account for 50–60% of individual miscarriages — but in RPL, the picture is more complex. After full investigation, chromosomal factors explain 30–40% of RPL cases; anatomical, immunological, and hormonal causes account for the remainder. This is why a comprehensive workup across all four cause domains is essential — a genetic explanation alone is correct in less than half of RPL cases.
What is PGT-A and how does it prevent miscarriage?
PGT-A (Preimplantation Genetic Testing for Aneuploidies) is a genetic test performed on IVF embryos before transfer. A small biopsy of cells is taken from the blastocyst, sent for chromosomal analysis, and only embryos with the correct number of chromosomes — confirmed euploid embryos — are transferred. Since chromosomal abnormality is the leading cause of miscarriage, transferring a confirmed-normal embryo dramatically reduces miscarriage risk — from 20–40% in unscreened cycles to 5–10% after PGT-A. At Wellspring IVF, PGT-A is available and recommended for appropriate RPL patients.
I have Antiphospholipid Syndrome — can I still have a successful pregnancy?
Yes — with the correct treatment, outcomes are excellent. Untreated APS carries a live birth rate of approximately 10–15% in RPL patients. With LMWH (Clexane) injections and low-dose aspirin commenced from a positive pregnancy test, live birth rates improve to 70–80%. APS is one of the most treatable causes of RPL — the treatment protocol is well-established, evidence-based, and has been used safely in pregnancy for decades.
My thyroid results were 'normal' — could thyroid still be causing my miscarriages?
Possibly — depending on what ‘normal’ means in your report. Standard laboratory reference ranges define TSH up to 4.5 mIU/L as normal. However, for fertility and early pregnancy, the evidence supports a target TSH below 2.5 mIU/L. A TSH of 3.5 mIU/L would be reported as ‘normal’ by most labs — but is associated with increased miscarriage risk. Dr. Shah always reviews the actual TSH value and anti-TPO antibodies — not just whether the result is flagged as abnormal.
We've had 3 losses and all our tests came back normal. What now?
‘Normal tests’ after RPL means you are in the unexplained RPL group — approximately 40–50% of RPL couples. This is frustrating, but it is not the end of options. First: empirical progesterone supplementation and aspirin are low-risk, evidence-informed options. Second, and most importantly: IVF with PGT-A removes the chromosomal variable entirely — even when parental karyotypes were normal. Mosaic embryos and low-grade aneuploidy are not detectable on parental blood tests but are found in embryos — PGT-A identifies them before transfer. For unexplained RPL with 3+ losses, PGT-A-assisted IVF is Dr. Shah’s primary recommendation.
Is IVF necessary for RPL, or can I try naturally after treatment?
IVF is not always necessary. If the cause of your RPL is anatomical (septum, polyps) — corrected by hysteroscopy — or immunological (APS) — managed with LMWH + aspirin — you may well conceive naturally or with IUI and carry successfully with the correct protocol in place. IVF with PGT-A is specifically recommended when: chromosomal cause is identified or strongly suspected, maternal age is >35–37 (where aneuploidy rates are high), or 3+ losses have occurred with no other treatable cause found.
How soon after a miscarriage can I try again?
Physically, the body typically recovers within one to two menstrual cycles after an early loss. However, Dr. Shah’s recommendation is: do not try again until the RPL investigation is complete and any treatable cause has been addressed. Attempting another pregnancy before treating APS, correcting a septum, or completing PGT-A creates a high probability of another loss — which serves no one. A 6–12 week investigation and treatment period is a worthwhile delay compared to another loss.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026