Low AMH Treatment in Ahmedabad — Your Own Eggs First, Always
“In my 15 years of treating fertility patients, the cases I find most rewarding are the women who arrive having been told their AMH is ‘too low’ for IVF. Low AMH is one of the most misunderstood reports in fertility medicine. A low number does not mean poor- quality eggs. I have seen women with AMH of 0.3 ng/mL achieve successful pregnancies with their own eggs through careful, personalised protocols. The answer is never to give up on your own eggs without a genuine effort.” — Dr. Pranay Shah, MS (ObGy), Director, Wellspring IVF & Women’s Hospital
Low AMH and Poor Ovarian Reserve — At a Glance
| Parameter | Details |
|---|---|
| Condition | Low AMH / Poor Ovarian Reserve (POR) |
| What AMH Measures | Egg quantity — the number of remaining follicles. NOT egg quality. |
| Normal AMH Range | 1.0 – 4.0 ng/mL (or 7.14 – 28.6 pmol/L) |
| Low AMH Definition | Below 1.0 ng/mL — indicates reduced ovarian reserve |
| Critical / Very Low | Below 0.5 ng/mL — requires specialist protocol |
| Our Core USP | “Own Eggs First” — we exhaust all options with your own eggs before any alternative is discussed |
| Key Protocols | Dual Stimulation (DuoStim) + Embryo Banking — for maximum egg collection |
| IVF Still Possible? | Yes — many women with low AMH achieve pregnancy with tailored IVF protocols |
| Specialist | Dr. Pranay Shah — 15+ Years | Advanced Poor Responder Protocols |
| Consultation | 📞 9099946050 | Free Second Opinion Available |
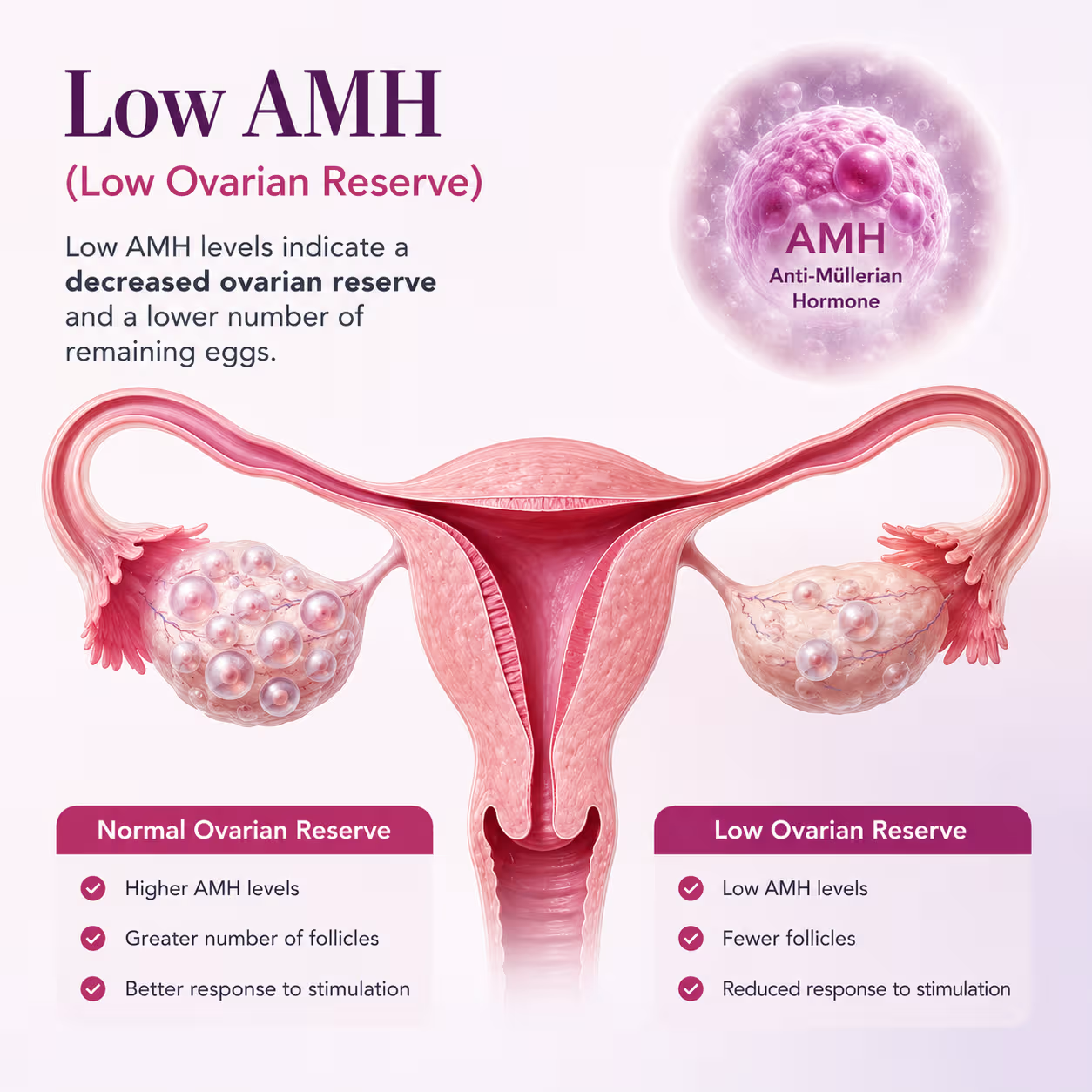
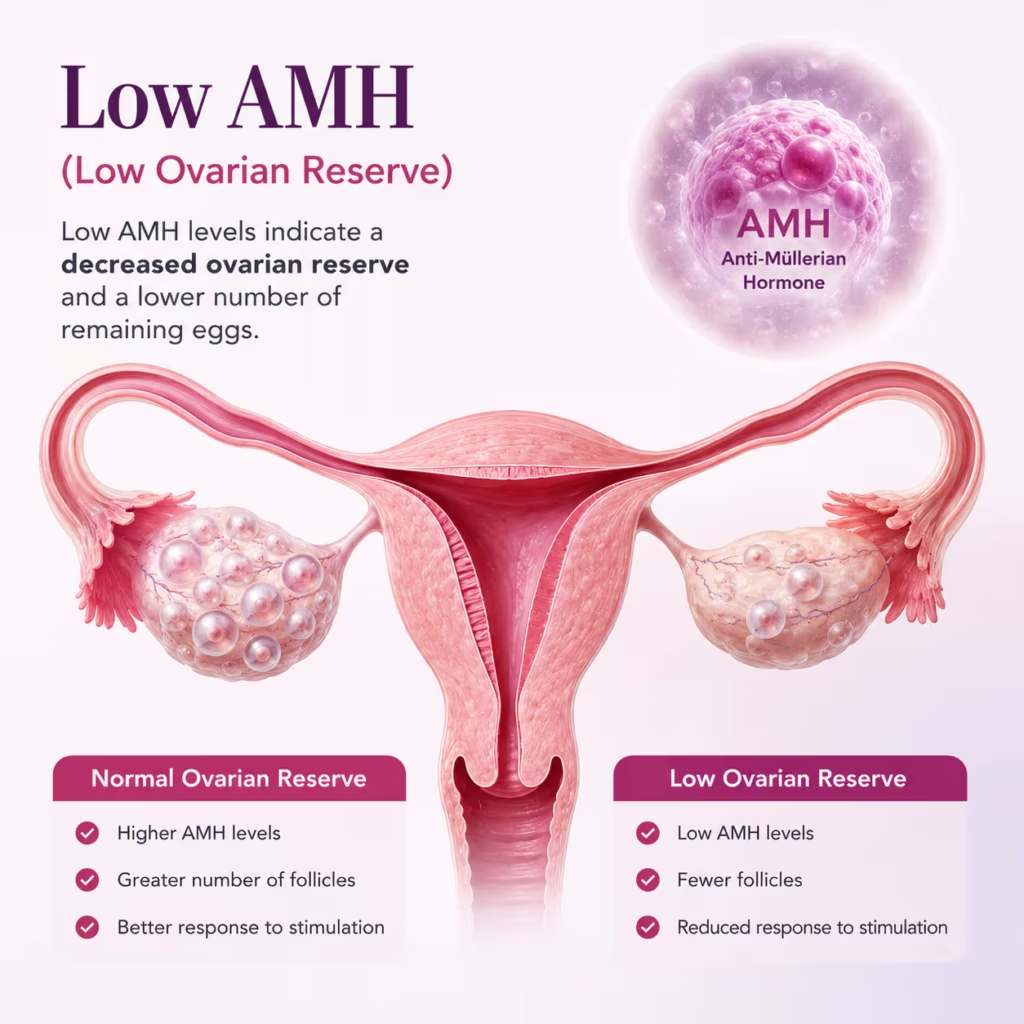
What Is AMH and What Does a Low Level Actually Mean?
Anti-Müllerian Hormone (AMH) is a protein hormone produced by the small follicles in the ovaries. Because these follicles contain the eggs that will eventually be recruited for ovulation, the level of AMH in the blood gives us an indirect measurement of how many eggs remain in the ovarian reserve — what fertility specialists call the ‘ovarian reserve.’
AMH is one of the most useful fertility blood tests because, unlike FSH or oestrogen, it does not fluctuate significantly during the menstrual cycle. This means it can be tested on any day of your cycle and gives a consistent, reliable picture of your remaining egg quantity.
Watch Our Low AMH Treatment Video
Learn how low AMH affects fertility, pregnancy chances, and the treatment options available to improve outcomes.
What You Will Learn
Understand fertility treatment options and pregnancy planning in low AMH cases.
- Low AMH and ovarian reserve
- Pregnancy chances with low AMH
- IVF options for low AMH
- Treatment planning and success factors
AMH Reference Ranges — What the Numbers Mean
| Category | AMH Level (ng/mL) | Fertility Implication |
|---|---|---|
| Optimal | Above 2.0 | Good egg reserve. Responds well to IVF stimulation. |
| Normal | 1.0 – 2.0 | Adequate reserve for IVF. Most patients respond well. |
| Low | 0.5 – 1.0 | Reduced reserve. Specialised IVF protocols recommended. Many successes possible. |
| Very Low | Below 0.5 | Significantly diminished reserve. Advanced poor-responder protocols required. Own eggs attempted first. |
The Most Important Thing to Understand: AMH Measures Quantity, NOT Quality
This is the most critical distinction in low AMH management, and one that is frequently misunderstood — even by some clinicians.
AMH tells us how many eggs you have remaining. It does not tell us about the genetic quality or developmental potential of those eggs. A woman with AMH of 0.4 ng/mL may have 3–4 eggs retrieved in an IVF cycle — but if those eggs fertilise normally and develop into good-quality embryos, the success rate per embryo transferred is not significantly different from a woman with a higher AMH.
The challenge with low AMH is not egg quality — it is egg quantity per cycle. Fewer eggs means fewer chances per stimulation. This is precisely why our advanced protocols (Dual Stimulation and Embryo Banking) exist: to maximise the total number of eggs collected, cycle by cycle, until we have enough good-quality embryos to attempt transfer.
What Causes Low AMH? Understanding the Root Cause
Low AMH can result from several different factors. Understanding the underlying cause matters, because it may influence the treatment approach:
- Age: The most common cause. AMH levels decline naturally and progressively from a woman’s mid-20s, with the steepest decline occurring from the mid-30s onward. This is a biological reality, not a disease.
- Endometriosis and Endometriomas: Chocolate cysts on the varies directly damage the surrounding follicular tissue, reducing AMH. Poorly performed cyst surgery can further reduce reserve. See our Endometriosis Treatment in Ahmedabad page for detail on reserve-protecting surgical approach.
- Previous Ovarian Surgery: Any surgery on the ovary — including cystectomy, ovarian drilling for PCOS, or surgery for torsion — can reduce the ovarian cortex and lower AMH.
- Cancer Treatment: Chemotherapy and pelvic radiotherapy are toxic to follicles and can cause rapid, severe reduction in AMH — sometimes leading to premature ovarian insufficiency.
- Autoimmune Conditions: The immune system can attack ovarian tissue in certain autoimmune conditions, reducing AMH over time.
- Genetics: A family history of early menopause (before age 45) is a significant predictor of earlier-than-normal decline in ovarian reserve.
- Idiopathic (Unknown Cause): In some women, particularly those under 35 with low AMH and no other identifiable cause, the reduction in reserve is unexplained. This is sometimes called Diminished Ovarian Reserve (DOR) and requires specialist management.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
The Wellspring Approach — Own Eggs First, Always
When a woman with low AMH comes to Wellspring IVF, the onversation does not begin with donor eggs. It begins with a thorough assessment of what her ovaries are genuinely capable of — and then with a protocol specifically designed to maximise that capability.
Dr. Pranay Shah has developed a structured approach for poor esponders that is used before any discussion of alternative options. This approach has two defining techniques:
Protocol 1: Dual Stimulation (DuoStim) — Two Chances in One Month
Dual Stimulation is one of the most significant advances in fertility treatment for poor responders in the past decade. It is based on a scientific observation: follicles do not grow only in the follicular phase of the cycle (days 1–14). The ovary can be stimulated to produce
additional eggs in the luteal phase (days 15–28) of the same cycle.
In a standard IVF cycle, stimulation is performed once — typically in the follicular phase. For a woman with low AMH who produces only 1–2 eggs in a standard cycle, this provides very limited material for embryo development.
In a DuoStim cycle, we stimulate twice:
- First stimulation: Standard follicular phase stimulation (days 1–14), egg collection, embryo development and vitrification (freezing).
- Second stimulation: Luteal phase stimulation begins approximately 5 days after the first egg collection (days 20–26 of the same cycle), collecting a second batch of eggs from the same month.
The result: in a single calendar month, we may collect double the number of eggs compared to a conventional single-stimulation cycle. For a poor responder, this can mean the difference between having 1–2 embryos and having 4–5 — a significant increase in the
cumulative probability of a successful pregnancy.
Current evidence shows that luteal phase-derived eggs have comparable fertilisation rates and embryo quality to follicular phase eggs. There is no compromise on quality — we are simply using a biological window that was previously left unexploited.
Protocol 2: Embryo Banking — Accumulating Your Best Chances
Embryo Banking (also called Embryo Accumulation) is a strategy where, rather than attempting an embryo transfer after every stimulation cycle, we vitrify (freeze) all embryos obtained across multiple cycles and accumulate them into a single cohort before any
transfer is attempted.
The logic is straightforward: for a woman with low AMH who produces 1–2 eggs per cycle, a single cycle may not yield enough embryos to achieve a transfer. But if we perform 2–3 stimulation cycles — often using DuoStim to maximise each month — and bank all the resulting blastocysts, we may accumulate 4–6 high-quality frozen embryos.
We then perform a single Frozen Embryo Transfer (FET) cycle in a well-prepared uterine environment, choosing the best embryo from the banked cohort. This strategy improves outcomes in several ways:
- Improves cumulative live birth rate compared to multiple single-embryo transfer attempts from individual cycles.
- Allows optional PGT-A (preimplantation genetic testing) on the banked embryo cohort before transfer, identifying the chromosomally normal embryo for transfer.
- Eliminates the risk of transferring into a stimulated uterine environment, which can be suboptimal for implantation after high-dose stimulation.
- Reduces patient anxiety by ensuring there is a good-quality embryo waiting before any transfer is attempted.
At Wellspring IVF, Dr. Pranay Shah carefully counsels each patient on whether DuoStim, Embryo Banking, or a combination of both is the most appropriate strategy for their specific AMH level, age, antral follicle count, and previous response history.
Ready To Begin Your IVF Journey?
The Complete Wellspring Toolkit for Poor Responders
Beyond Dual Stimulation and Embryo Banking, Dr. Shah uses a comprehensive set of evidence-based interventions for women with low AMH:
- Individualised stimulation protocols: Standard antagonist protocols are often not optimal for poor responders. Dr. Shah may use modified protocols such as the ‘Bologna criteria’ protocol, mini-IVF, or modified natural cycle IVF depending on AMH level and previous response.
- DHEA supplementation: Dehydroepiandrosterone (DHEA), typically 25–75 mg daily for 6–12 weeks before an IVF cycle, has evidence supporting improved ovarian response and egg quality in poor responders. It is prescribed selectively based on individual assessment.
- CoQ10 supplementation: Coenzyme Q10 supports mitochondrial function in oocytes, potentially improving egg quality. 200–600 mg daily for 2–3 months before IVF is often recommended for women over 35 with low reserve.
- Growth Hormone co-treatment: In selected poor responders, Growth Hormone (GH) is added to the IVF stimulation protocol. Evidence suggests it can improve ovarian response and egg yield in women who have previously had a poor response to standard stimulation.
- Antral Follicle Count (AFC) correlation: AMH is always interpreted alongside AFC on ultrasound. Sometimes AMH is disproportionately low relative to the visible follicle count — in such cases, the ovarian response may be better than the AMH level suggests.
- Natural Cycle IVF: For women with very low AMH (below 0.3 ng/mL) who produce very few follicles even with stimulation, Natural Cycle IVF — collecting the single naturally selected dominant egg each month — may offer a gentle, cost-effective way to accumulate embryos without the side effects of high-dose stimulation.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
When Own Eggs Are No Longer Sufficient — Understanding Your Options Under the ART Act 2022
For the overwhelming majority of women with low AMH, the strategies above provide a genuine and often successful path to pregnancy with their own eggs. However, we believe in honest, transparent counselling — and there are situations where, after an exhaustive and genuine attempt with own eggs, the likelihood of success becomes very low.
In such circumstances, Dr. Shah will have a full, unhurried conversation about the remaining pathways. At Wellspring IVF, this conversation is always factual, never pressured, and always led by what is in your best interest — not by commercial considerations.
Donor Egg IVF — Important Information Under the ART (Regulation) Act, 2022
In India, the use of donor eggs in assisted reproduction is strictly regulated by the Assisted Reproductive Technology (Regulation) Act, 2022, and the rules framed thereunder. At Wellspring IVF, we follow these regulations completely and without exception.
Under the ART Act 2022, oocyte (egg) donation is permitted only through a registered ART Bank. Key provisions that patients must understand:
- Donor source: Eggs can only be obtained from registered, voluntary oocyte donors through an ART Bank registered under the ART Act 2022. Direct or known donation between individuals is not permitted under the Act.
- Voluntary donation: All donors are voluntary — they have provided informed consent to donate oocytes through the registered ART Bank system. Donors are never coerced or commercially exploited.
- Donor anonymity: Donor identity is maintained as per the provisions of the ART Act. The child born has the right to access non-identifying medical information about the donor.
- Medical screening: All donors registered with the ART Bank undergo comprehensive medical, genetic, and psychological screening as mandated by the Act.
- Matching: Matching between donor and recipient is performed considering physical characteristics as permitted under the Act and its guidelines.
We understand that reaching this conversation is emotionally significant. Dr. Shah and our counselling team will guide you through every aspect of this process — the medical procedure, the legal framework, the emotional considerations, and the realistic success rates — with complete transparency and compassion.
Related Conditions We Commonly Evaluate Alongside Low AMH
Low AMH sometimes occurs alongside other fertility conditions. A complete evaluation at Wellspring IVF ensures nothing is overlooked:
- Endometriosis — endometriomas directly damage ovarian tissue and reduce AMH. Reserve-protecting surgery is critical if intervention is needed.
- PCOD and PCOS — PCOS patients typically have high AMH (many follicles), but occasionally older PCOS patients can have declining reserve. Hormonal context must be evaluated separately.
- Uterine Fibroids — can impair implantation even when a good embryo is obtained through low AMH protocols.
- Blocked Fallopian Tubes — if tubes are blocked, IVF is the necessary route, making efficient egg collection from low-reserve ovaries even more critical.
- Male Factor Infertility — when both low AMH and a sperm issue are present simultaneously, the treatment strategy must be coordinated. See our Azoospermia Treatment and Oligospermia Treatment pages.
Frequently Asked Questions
Can I get pregnant naturally with low AMH?
Yes — low AMH reduces the probability of natural conception because there are fewer follicles recruited each cycle, meaning the chance of spontaneous ovulation producing a viable egg in any given month is lower. However, it does not make natural conception impossible. Many women with AMH below 1.0 ng/mL conceive naturally. The key factors are age, egg quality, partner’s sperm parameters, and tubal health.
Does low AMH mean my eggs are poor quality?
No — this is the most important misconception to address. AMH measures the quantity of your remaining follicles, not the genetic or developmental quality of your eggs. A woman with low AMH can have excellent-quality eggs. Egg quality declines with age, but this is a separate biological process from the decline in AMH. Two women aged 32 with the same low AMH level will typically have similar egg quality. The challenge is the smaller number of eggs available per cycle.
What is Dual Stimulation (DuoStim) and is it safe?
Dual Stimulation involves two separate ovarian stimulations within a single menstrual cycle — one in the follicular phase and one in the luteal phase. It is well-supported by clinical evidence published in peer-reviewed reproductive medicine journals. Current data shows that luteal phase oocytes have comparable fertilisation rates and embryo developmental competence to follicular phase oocytes. The approach is considered safe and is specifically designed for poor responders who need to maximise egg yield per month.
How many IVF cycles will I need with low AMH?
This varies significantly based on your specific AMH level, age, antral follicle count, and how your ovaries respond to stimulation. Some patients accumulate enough embryos in a single DuoStim cycle. Others benefit from 2–3 banking cycles before transfer. Dr. Shah will discuss a realistic expectation at your first consultation based on your complete diagnostic picture — not a one-size-fits-all estimate.
Is DHEA supplementation scientifically proven for low AMH?
DHEA supplementation has a growing body of evidence supporting its use in diminished ovarian reserve. Several randomised controlled trials and meta-analyses have reported improved ovarian response, higher egg yields, and better embryo quality in poor responders who supplement with DHEA for 6–12 weeks before IVF. It is not effective for every patient, and Dr. Shah prescribes it selectively based on individual assessment rather than as a blanket recommendation.
At what AMH level should I consider IVF immediately rather than trying naturally?
There is no absolute threshold, but the general principle is this: time is a significant factor in low AMH. Since the ovarian reserve continues to decline, delay can be costly. Women under 35 with AMH between 0.5–1.0 ng/mL may have 6–12 months to attempt natural conception before pursuing IVF, depending on other factors. Women over 35, or with AMH below 0.5 ng/mL, are generally advised to pursue IVF without significant delay. Dr. Shah will give you a personalised recommendation at consultation.
What if I have been turned away by another clinic because of my low AMH?
Unfortunately, some fertility centres use AMH thresholds as a reason to decline treatment with own eggs. At Wellspring IVF, we do not operate this way. We evaluate every patient individually, consider the complete clinical picture, and offer a genuine trial with own eggs using our advanced protocols before any alternative is discussed. Many of our most rewarding outcomes are in patients who were told elsewhere that their situation was hopeless.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026

Take the Next Step — Your Own Eggs Deserve a Genuine Chance
A low AMH result is the beginning of a conversation — not the end of a journey.