Female Infertility Treatment in Ahmedabad | Causes & Diagnosis | Wellspring IVF
At Wellspring IVF & Women's Hospital, we believe that successful treatment begins with precise diagnosis. Infertility is not a single disease; it is a symptom of an underlying condition. It could be hormonal (like PCOD), structural (like blocked tubes), or related to egg reserve (Low AMH). Treating "infertility" without identifying the specific cause is like trying to drive to a destination without a map. we provide comprehensive female infertility treatment in Ahmedabad that targets the root cause of your struggles—whether it is ovulation induction for PCOS, advanced laparoscopy for endometriosis, or tailored IVF protocols for low AMH.
Dr. Pranay Shah leads one of Gujarat's most comprehensive female fertility programs. We do not believe in "unexplained infertility" as a final answer. We believe in digging deeper — using advanced ultrasound, hormonal profiling, and diagnostic laparoscopy — to find the root cause and treat it directly.
The 4 Pillars of Female Fertility: What We Check
Ovulation — The Egg Release
- The Requirement: You must release a mature, healthy egg from your ovary once a month.
- The Problem: Hormonal imbalances prevent the egg from maturing or releasing.
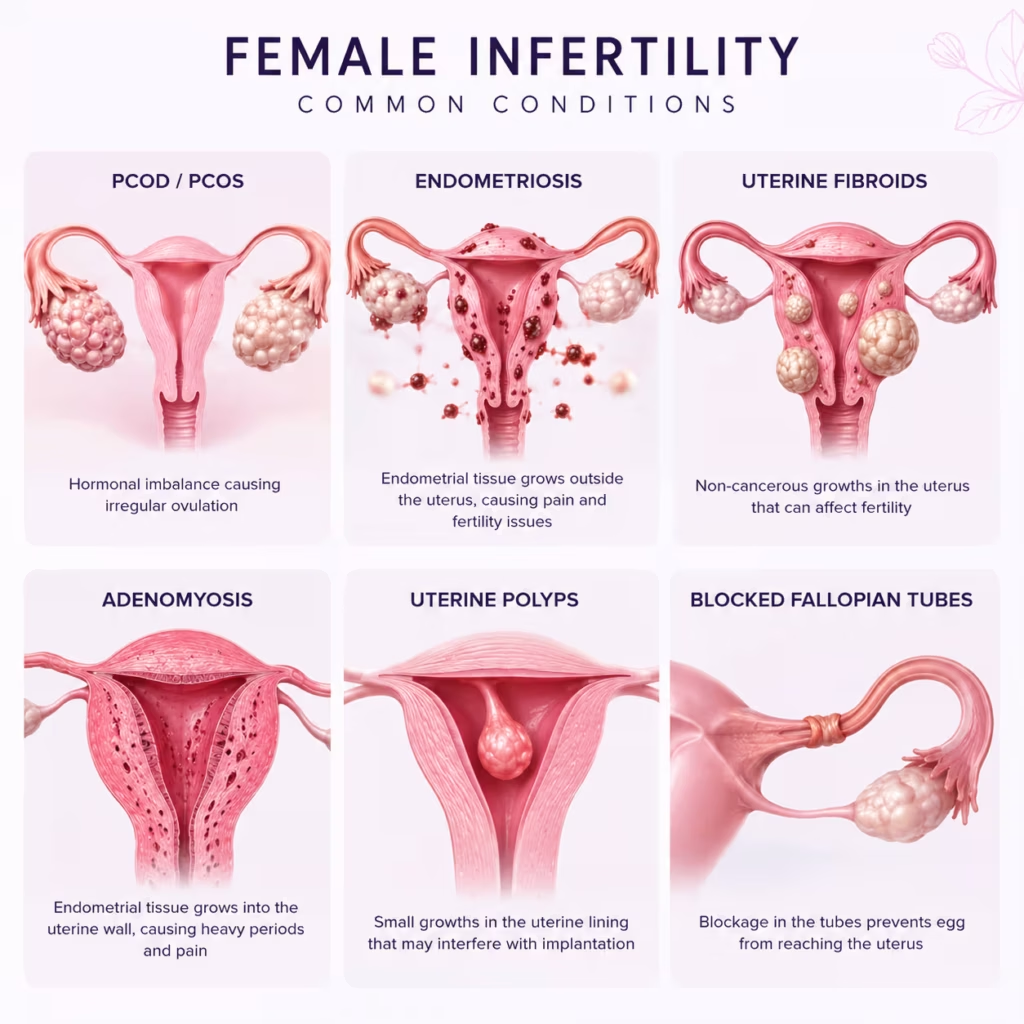
- Common Conditions: PCOD / PCOS | Thyroid issues | Hyperprolactinaemia
Tubal Patency — The Transport
- The Requirement: The fallopian tubes must be open and healthy to catch the egg and allow sperm to reach it.
- The Problem: Blockages prevent the sperm and egg from meeting.
- Common Conditions: Blocked Fallopian Tubes | Hydrosalpinx | Pelvic TB
Uterine Environment — The Home
- The Requirement: The uterus must be healthy, with a receptive lining for the embryo to implant.
- The Problem: Growths or structural issues prevent implantation or cause miscarriage.
- Common Conditions: Uterine Fibroids | Adenomyosis | Polyps | Uterine Septum
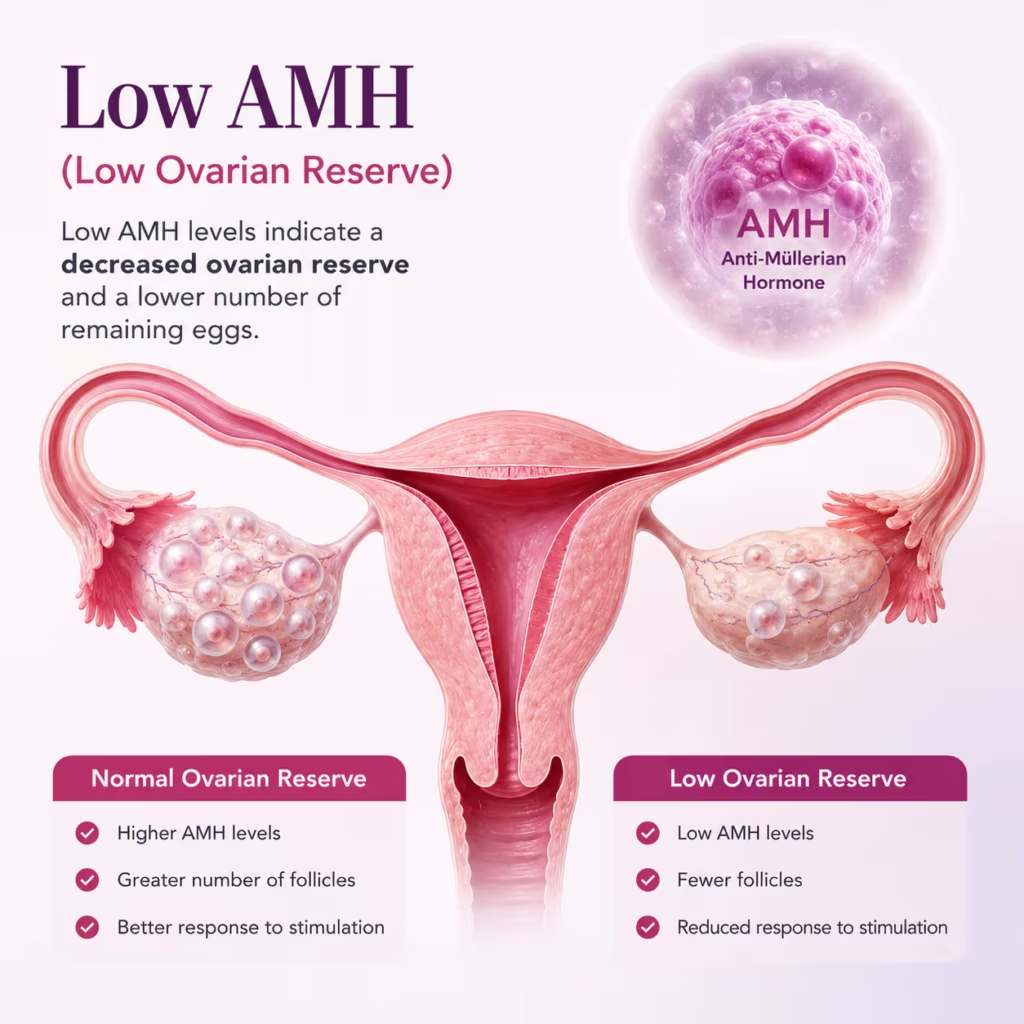
Ovarian Reserve — The Quantity
- The Requirement: You must have a sufficient number of remaining eggs for your age.
- The Problem: Egg numbers are critically low, reducing the monthly chance of conception.
- Common Conditions: Low AMH / Poor Ovarian Reserve | Premature Ovarian Insufficiency
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Symptom Navigator: What Is Your Body Telling You?
| If You Experience… | It Could Indicate… | Recommended Page |
|---|---|---|
| Irregular periods, weight gain, acne, facial hair | PCOD / PCOS | Read More → |
| Severe period pain, pain during sex, chronic pelvic pain | Endometriosis | Read More → |
| Heavy bleeding, prolonged periods, pelvic pressure | Fibroids / Adenomyosis | Read More → |
| No symptoms, but history of pelvic infection or surgery | Blocked Tubes | Read More → |
| Short cycles (<25 days), age over 35, family history of early menopause | Low AMH | Read More → |
| Multiple pregnancy losses (2 or more) | Recurrent Miscarriage | Consult Dr. Shah |
How We Diagnose Female Infertility at Wellspring
We do not waste time. Your first consultation with Dr. Pranay Shah includes a thorough review of your history and a clear diagnostic plan.
Advanced Transvaginal Ultrasound (TVS)
Dr. Shah personally performs a high-resolution scan to assess your uterus, ovarian volume, and Antral Follicle Count (AFC). This gives us an immediate picture of your structural health and egg reserve.
Hormonal Profiling
We check key hormones (AMH, FSH, LH, TSH, Prolactin) to understand your ovulatory function and egg quantity.
Tubal Evaluation (HSG)
If tubes have not been checked, we perform an HSG (dye test) to confirm they are open.
Diagnostic Laparoscopy / Hysteroscopy
For complex cases — suspected endometriosis or uterine septum — we use minimally invasive keyhole diagnostic surgery (Diagnostic Laparoscopy or Diagnostic Hysteroscopy) to see exactly what is happening inside.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Ready for Complete Fertility Diagnostic Clarity?
Myth vs. Fact: "My Periods Are Regular, So I Can't Be Infertile"
The “Regular Period” Trap
Many women believe that if they get a period every month, their fertility is fine. This is false.
- You can have regular periods and still have Blocked Tubes.
- You can have regular periods and still have Endometriosis.
- You can have regular periods and have Low Egg Quality.
Regular menstruation only tells us one thing: you are ovulating. It does not tell us if the egg can meet the sperm, or if the embryo can implant. Do not delay testing just because your cycle is regular.
Treatment Pathways: From Simple to Advanced
We always start with the least invasive effective treatment. We do not push everyone to IVF.
- For Ovulation Issues (PCOD): We start with Ovulation Induction (tablets / injections) and timed intercourse. Read more: PCOD / PCOS Treatment.
- For Mild Male Factor / Unexplained Infertility: We try IUI Treatment — placing sperm directly in the uterus.
- For Blocked Tubes / Severe Endometriosis / Low AMH: We move to IVF Treatment or ICSI to bypass the problem and maximise success.
- For Uterine Issues: We perform corrective Laparoscopic Surgery to restore the anatomy before attempting pregnancy.
“I see women who have been given Clomid for 6 months without a single scan to check if they are even ovulating. I see women with silent endometriosis that has never been detected — not because it was hidden, but because nobody looked. My promise to every patient is simple: we will look. We will find the real answer. And then we will treat it — not guess at it.”
— Dr. Pranay Shah, iop[ MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
Frequently Asked Questions
How do I know if my fallopian tubes are blocked if I have no symptoms?
Fallopian tube blockages rarely cause physical symptoms, pain, or changes in your menstrual cycle. Most women only discover a blockage after experiencing difficulty conceiving. The most definitive and reliable way to check tubal health is through a diagnostic test called a Hysterosalpingography (HSG)—a specialized X-ray dye test—or via a minimally invasive diagnostic laparoscopy. If you have a history of pelvic infections, severe bursts of pelvic pain, or past abdominal surgeries, proactive tubal testing is highly recommended.
Does a low AMH level mean my egg quality is also poor?
Not necessarily. Anti-Müllerian Hormone (AMH) measures egg quantity (your remaining ovarian reserve), not egg quality. A woman can have a low AMH level but still have highly viable, healthy eggs that can lead to a successful pregnancy, especially if she is younger. While a lower AMH means there are fewer follicles available during an IVF stimulation cycle, the focus shifts from quantity to maximizing the health of the remaining eggs through tailored medical protocols.
Can I get pregnant naturally if I have severe Endometriosis or Adenomyosis?
While both conditions create an inflammatory environment that can hinder conception, natural pregnancy is still possible depending on the severity. Endometriosis can physically distort pelvic anatomy or block tubes, while Adenomyosis primarily impacts the uterine lining’s receptivity. For mild cases, natural conception or simple treatments may work. However, for moderate-to-severe cases, advanced treatments like down-regulation therapy followed by IVF or corrective laparoscopic surgery are often the most successful routes to bypass the inflammatory barrier.
Is it possible to have regular periods but still not release an egg (Anovulation)?
Yes, this is a clinical reality known as an anovulatory cycle. You can experience regular, monthly bleeding that looks exactly like a normal period without actually releasing a mature egg. This happens when the uterine lining builds up normally under estrogen but eventually sheds due to hormonal fluctuations rather than progesterone withdrawal post-ovulation. Tracking through ovulation predictor kits (OPKs), monitoring basal body temperature, or performing a simple day-21 progesterone blood test can confirm if true ovulation is taking place.
How long after treating uterine fibroids or polyps can I try to conceive?
The recovery timeline depends entirely on the size, location, and method used to remove the growths. For minor endometrial polyps removed via a simple hysteroscopy, couples can often safely start trying to conceive within 1 to 2 menstrual cycles. For larger intramural or submucosal fibroids requiring a myomectomy, the uterine muscle needs deeper healing, and a waiting period of 3 to 6 months is typically advised to ensure the uterine environment is perfectly strong enough to support a growing pregnancy.
How does a thyroid imbalance directly impact my ability to get pregnant?
Your thyroid hormones interact directly with your reproductive hormones (estrogen and progesterone). Both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) can disrupt the luteinizing hormone (LH) surge, leading to irregular ovulation or poor egg maturation. Additionally, poorly managed thyroid levels can interfere with the luteal phase, making it difficult for a fertilized embryo to implant securely in the uterus, increasing the risk of early pregnancy loss. Balancing TSH levels with medication is a quick and effective fertility booster.
What is the difference between PCOS and PCOD, and do they affect fertility differently?
hile closely related, PCOD (Polystic Ovarian Disease) is a more common, milder condition where the ovaries produce immature eggs due to a temporary hormonal imbalance, which can often be managed effectively with lifestyle corrections and targeted medication. PCOS (Polycystic Ovarian Syndrome) is a more severe, systemic metabolic disorder where the ovaries produce higher levels of male hormones (androgens), causing ovulation to stop altogether alongside metabolic symptoms like insulin resistance. Both impact fertility by disrupting regular egg release, but PCOS typically requires a more comprehensive clinical protocol, such as specialized ovulation induction or advanced IVF planning, to achieve pregnancy.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026