ICSI Treatment in Ahmedabad
Request a Free Callback
For couples facing male infertility — low sperm count, poor motility, abnormal morphology, or even the complete absence of sperm in the ejaculate — the question of how fertilisation can possibly occur feels overwhelming. ICSI (Intracytoplasmic Sperm Injection) is the answer that has transformed male factor infertility from a near-insurmountable barrier into a highly treatable condition.
ICSI is an advanced IVF laboratory technique in which a single, carefully selected sperm is directly injected into the centre of a mature egg using an ultra-fine glass needle — a micropipette. Unlike conventional IVF — where thousands of sperm must naturally penetrate the egg — ICSI removes the entire competitive process of fertilisation and replaces it with precision science. At Wellspring IVF, ICSI is performed by our dedicated in-house embryology team under Dr. Pranay Shah’s direct supervision using precision micromanipulation equipment. We do not outsource embryology. Your embryos are handled in-house, at every step.
70–80%
80%+
1 Sperm
15+ Yrs
6,000+
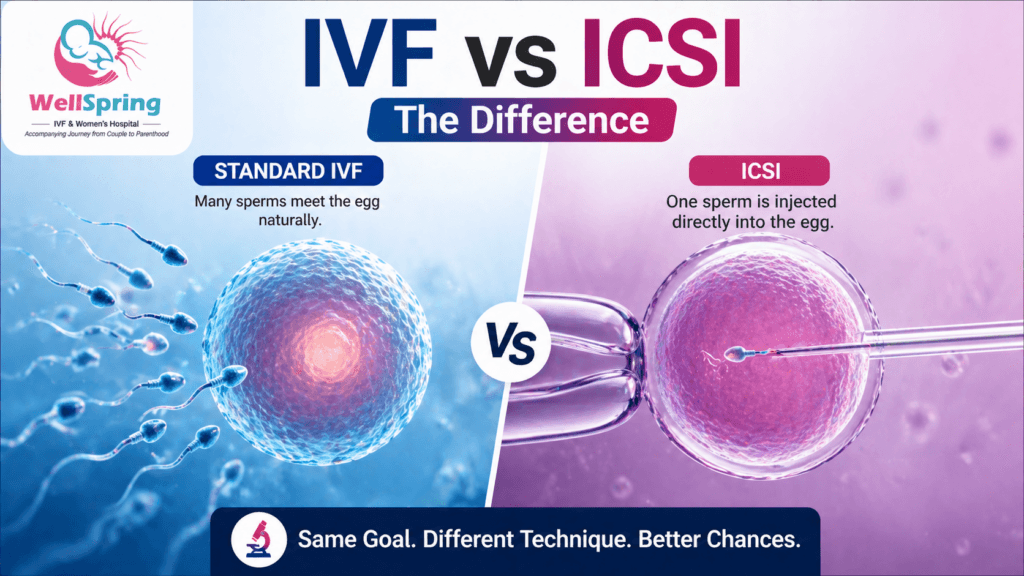
Standard IVF vs ICSI —
Why the Difference Matters Enormously
To understand why ICSI is so significant, you need to understand what standard IVF requires of the sperm — and precisely where it fails in male factor infertility cases. The following comparison is the single most important distinction you need to grasp before understanding your treatment options.
| Comparison Point | Standard IVF | ICSI |
|---|---|---|
| Fertilisation method | Sperm placed near egg — must penetrate zona pellucida naturally | Single sperm injected directly into egg cytoplasm by embryologist |
| Sperm quantity required | 50,000–100,000+ motile sperm per egg | Only ONE viable sperm per egg |
| Motility requirement | Sperm must swim to reach and penetrate the egg | Even immotile sperm can be used — motility is not required |
| Where it fails | Fails when sperm count is very low, motility severely reduced, or penetration impossible | Eliminates all competitive fertilisation barriers entirely |
| Fertilisation rate | 50–70% when sperm quality is normal | 70–80% regardless of sperm quality — embryologist controls fertilisation |
| Best suited for | Normal semen parameters or mild male factor | Low count, poor motility, poor morphology, azoospermia, failed fertilisation history |
Who Needs ICSI? —
Clinical Indications for ICSI Treatment in Ahmedabad
ICSI is recommended whenever natural fertilisation — even in a standard IVF setting — is unlikely to succeed, or when there is a documented history of fertilisation failure. Dr. Pranay Shah evaluates the complete semen analysis, previous treatment history, and female factor findings before recommending ICSI. Below are the primary indications we treat at Wellspring IVF.
Oligospermia (Low Sperm Count)
Total sperm count below 15 million/mL or total motile count below 5 million makes natural fertilisation unreliable. ICSI bypasses the competitive fertilisation process entirely, requiring only one viable sperm per egg.
Asthenospermia (Poor Sperm Motility)
When progressive motility is below 32%, sperm cannot physically reach and penetrate the egg in standard IVF. ICSI requires only viability — not swimming ability — making poor motility irrelevant to the fertilisation outcome.
Teratospermia (Abnormal Sperm Morphology)
When normal-form sperm is below 4% on Kruger strict criteria, penetration of the zona pellucida is severely impaired. The ICSI embryologist hand-selects the most structurally intact sperm from the entire sample — morphological failure of the majority does not prevent fertilisation.
Azoospermia (Zero Sperm in Ejaculate)
When no sperm is present in the ejaculate — whether due to obstruction (Obstructive Azoospermia) or production failure (Non-Obstructive Azoospermia) — sperm is surgically retrieved via TESE or PESA. ICSI is the only technique that can utilise these surgically retrieved sperm, which are always present in very small numbers.
High Sperm DNA Fragmentation (DFI > 25%)
When sperm DNA integrity testing reveals a Fragmentation Index above 25–30%, even morphologically normal sperm may carry damaged genetic material that compromises embryo development. ICSI combined with PICSI or IMSI selects sperm at a deeper biological level — beyond what standard ICSI selection can assess.
Previous Total Fertilisation Failure (TFF)
If a previous standard IVF cycle resulted in zero fertilisation despite adequate egg numbers and apparently normal sperm quality, ICSI is mandated for all subsequent cycles. Something in the natural fertilisation process failed — ICSI removes that variable entirely.
Frozen or Surgically Retrieved Sperm
Sperm that has been cryopreserved experiences reduced motility after thawing. Sperm extracted from the testis or epididymis via TESE or PESA is present in tiny quantities. ICSI is always the technique of choice in both scenarios — it does not require high sperm numbers or normal motility to achieve reliable fertilisation.
WHO Reference — Semen Parameters That Indicate ICSI
The following WHO 2021 lower reference limits represent the 5th percentile of fertile men. Values below these thresholds, combined with difficulty conceiving, are sufficient indication for ICSI at Wellspring IVF:
Total Sperm Count: < 39 million per ejaculate | Sperm Concentration: < 16 million/mL
Progressive Motility: < 30% | Total Motility: < 42%
Normal Morphology (Kruger): < 4% | Sperm DNA Fragmentation Index: > 25% (high-risk threshold)
Any single parameter falling below reference — combined with fertility difficulty — is a sufficient indication for ICSI at Wellspring IVF.
Watch Our ICSI Treatment Video
Learn how ICSI treatment works, when it may be recommended, and what couples can expect during the process.
What You Will Learn
Learn how ICSI treatment works, when it may be recommended for male infertility, and what couples can expect during the fertility treatment process.
- How ICSI differs from conventional IVF
- Male infertility conditions requiring ICSI
- Fertilization and embryo development process
- ICSI success factors and treatment basics
The ICSI Procedure —
Step by Step Inside Wellspring's IVF Laboratory
Sperm Preparation —
Finding the Best Candidate
On the morning of OPU, the male partner provides a semen sample (or the pre-frozen / surgically retrieved sample is thawed). The sample is processed using density gradient centrifugation and swim-up separation to isolate the most motile, morphologically normal sperm from seminal plasma, debris, and dead cells. The final washed preparation represents the elite fraction of the sample — only these are available for ICSI injection.
Egg Assessment —
Identifying Mature Eggs Ready for ICSI
Eggs retrieved from follicles during OPU are immediately evaluated by our embryologist. Only MII (Metaphase II) eggs — mature, fully developed eggs — are suitable for ICSI. Immature (MI or GV) eggs are identified and set aside. The number of MII eggs is recorded and communicated to Dr. Shah — this determines how many ICSI injections will be performed.
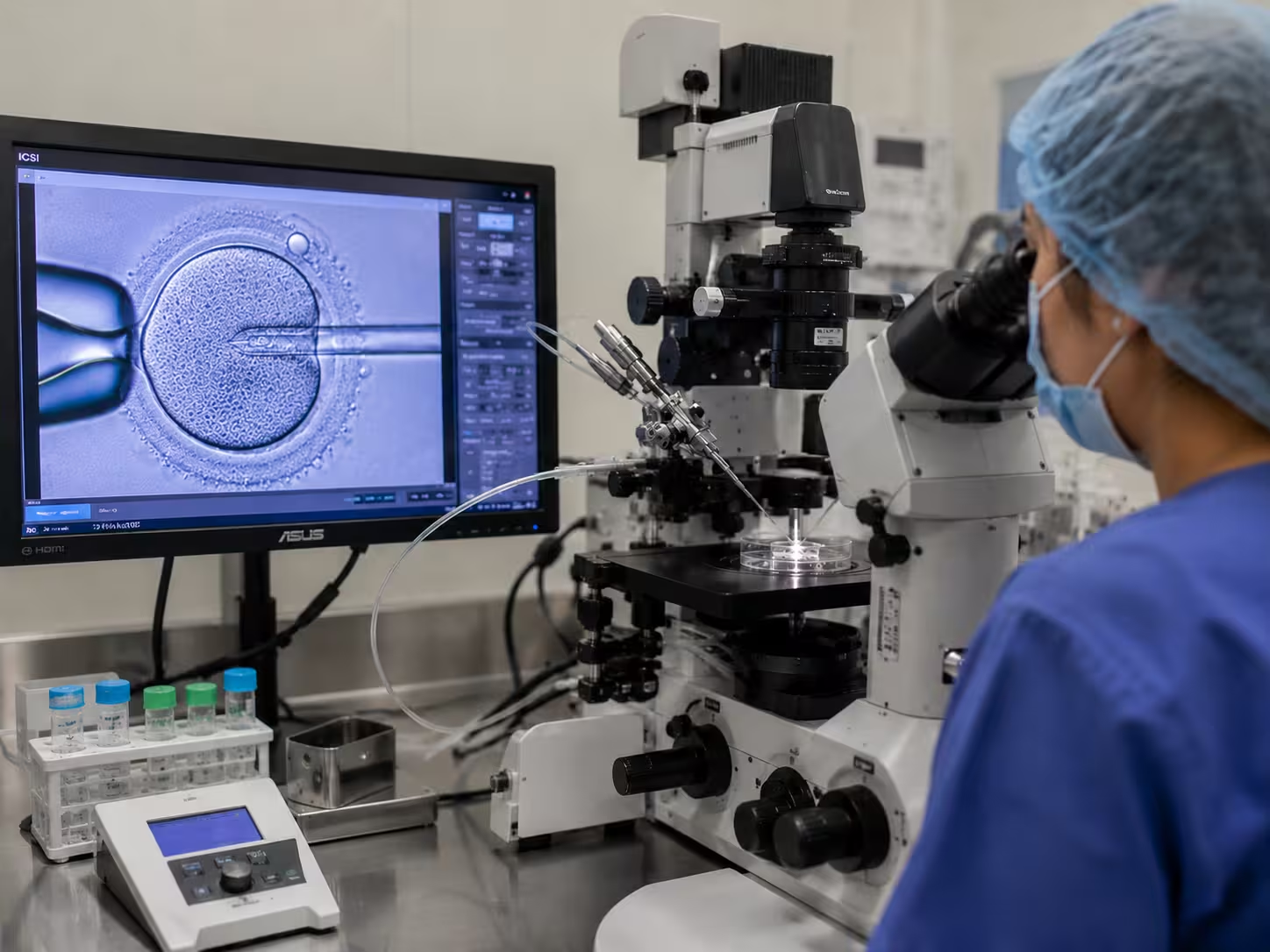
ICSI Injection —
Precision Under the Microscope
Each mature egg is placed in a micromanipulation dish under the high-powered microscope. A holding pipette secures the egg gently. The embryologist then uses the fine micropipette needle — thinner than a human hair — to pick up a single selected sperm, immobilise it, and inject it directly through the zona pellucida and into the egg cytoplasm. This process takes approximately 30–60 seconds per egg and requires exceptional technical precision.
Post-Injection Culture —
Confirming Fertilisation
After injection, eggs are placed in our advanced incubation system replicating the natural fallopian tube environment precisely — controlled temperature, CO₂ concentration, and humidity. Fertilisation is confirmed the following morning (Day 1) by checking for the appearance of two pronuclei (2PN) inside the egg — one from the sperm, one from the egg. 2PN confirmation = successful fertilisation and the beginning of embryo development.
Embryo Development —
Days 2 to 5
Fertilised eggs are cultured to either Day 3 (8-cell cleavage stage) or Day 5/6 (blastocyst stage) depending on your specific protocol. Blastocyst culture is performed at Wellspring in the majority of cases — Day 5 embryos have significantly higher implantation potential than Day 3 embryos and allow for better embryo selection before transfer.
Embryo Selection and Transfer
On Day 3 or Day 5, our embryologist grades each embryo on standardised morphological criteria. The best-quality embryo is recommended for transfer. Additional high-grade embryos are vitrified (freeze-preserved) for future cycles if needed. Dr. Pranay Shah personally performs every embryo transfer at Wellspring — with ultrasound guidance for optimal placement accuracy.
Going Beyond ICSI — Learn About High-Magnification IMSI and PICSI
IMSI — Intracytoplasmic Morphologically Selected Sperm Injection
IMSI is Recommended When:
- Standard ICSI cycles have produced embryos of consistently poor quality despite adequate egg numbers
- Sperm morphology is severely abnormal even on standard analysis (teratospermia <1% normal forms)
- Two or more ICSI cycles have ended in failed fertilisation or poor blastocyst development
- Recurrent implantation failure where the male factor has not been fully excluded
PICSI — Physiological Intracytoplasmic Sperm Injection
PICSI is Recommended When:
- Sperm DNA fragmentation testing (DFI) reveals a fragmentation index above 25–30%
- Previous IVF / ICSI cycles have produced embryos that arrest early in development
- Recurrent implantation failure where sperm DNA integrity has not been assessed
- Male partner age > 40 years with elevated concern about sperm DNA integrity
| Feature / Indicator | ICSI | IMSI | PICSI |
|---|---|---|---|
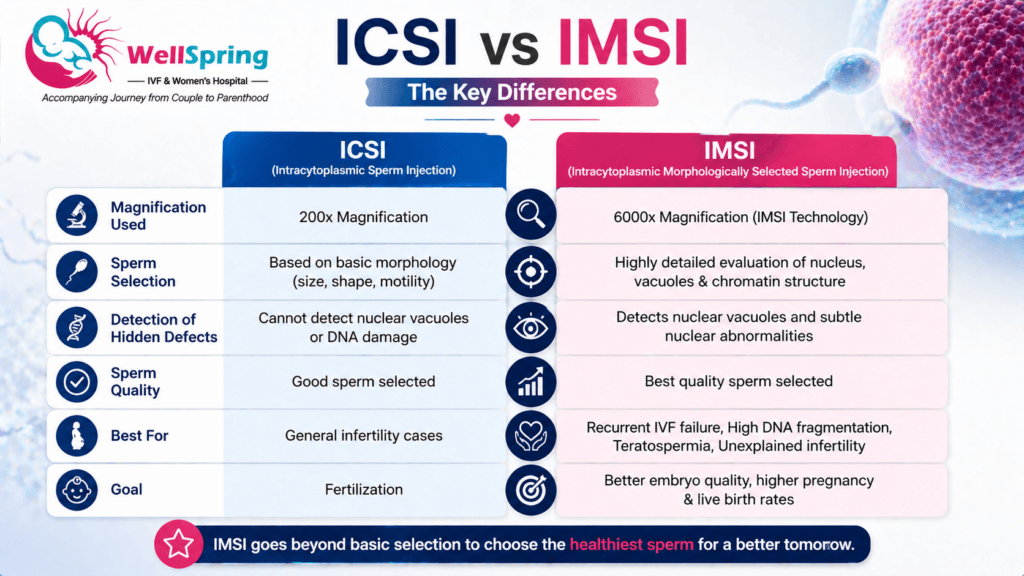
| Magnification | 200–400× | 6,000–10,000× | Standard + hyaluronan binding |
| Nuclear vacuole check | Not possible | Yes — visible & excluded | Partial — via maturity marker |
| DNA fragmentation | Not addressed | Partially mitigated | Directly targeted |
| Best for | Most ICSI cases | Poor morphology, poor embryo quality | High DFI, recurrent failure |
| Available at Wellspring | Yes — standard | Yes — on indication | Yes — on indication |
Ask Dr. Shah Whether IMSI or PICSI Is Right for Your Case
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
ICSI for Azoospermia — When There Is No Sperm in the Ejaculate
| Obstructive Azoospermia (OA) | Non-Obstructive Azoospermia (NOA) |
|---|---|
| Cause: Blockage in vas deferens or epididymis prevents sperm from reaching the ejaculate | Cause: Testicular production failure — sperm are not being produced in sufficient numbers |
| Sperm retrieval: PESA or conventional TESE — sperm found in almost all cases | Sperm retrieval: Micro-TESE — requires surgical search under microscope magnification |
| ICSI success with retrieved sperm: Comparable to ejaculated sperm ICSI rates | Sperm found in approximately 40–60% of Micro-TESE cases; ICSI success when found is comparable |
| Examples: Post-vasectomy, CBAVD, prior epididymal infection | Examples: Klinefelter syndrome (47,XXY), Y-chromosome microdeletion, spermatogenic arrest |
Pre-ICSI Evaluation for Azoospermia — What Dr. Shah Recommends
- Hormonal Profile: FSH, LH, Total Testosterone, Prolactin — to differentiate obstructive from non-obstructive cause
- Karyotype (chromosomal analysis): To rule out Klinefelter syndrome (47,XXY) and other chromosomal causes
- Y-chromosome Microdeletion Testing: AZF region deletions — AZFa and AZFb deletions predict Micro-TESE failure
- Testicular Volume Assessment: By ultrasound — small testes with high FSH suggests NOA
Full details : Azoospermia — Diagnosis, TESE, and ICSI at Wellspring IVF
Start Your ICSI Journey Today
ICSI Success Rates — What to Realistically Expect
| Outcome Measure | Typical Range |
|---|---|
| Fertilisation rate per MII egg | 70–80% (Wellspring) vs 60–70% industry standard |
| Blastocyst formation rate (Day 5) | 40–60% of fertilised embryos reach blastocyst stage |
| Clinical pregnancy rate per transfer | 40–65% (varies with age, diagnosis, embryo grade) |
| Live birth rate per transfer (age < 35) | 50–60% with good-quality blastocyst transfer |
| Live birth rate per transfer (age > 38) | 25–40% — declines significantly with female age |
| Cumulative live birth rate (2–3 cycles) | 70–80% for patients with good ovarian response |
Important: How to Interpret These Numbers
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan

ICSI Cost in Ahmedabad — Transparent Pricing at Wellspring IVF
A complete, itemised quotation including IVF stimulation medications, laboratory charges, ICSI fee, embryo culture costs, and transfer fee is provided at your initial consultation with Dr. Pranay Shah. For our detailed IVF and ICSI cost breakdown, visit our master IVF hub page or call our team directly.
What Is Included in the ICSI Quotation at Wellspring
- Ovarian stimulation monitoring (follicular scans + blood tests during stimulation)
- OPU (Egg retrieval) — procedure, anaesthesia, and operating room charges
- Semen processing and sperm preparation on the day of OPU
- ICSI laboratory procedure — embryologist time, micromanipulation equipment, injection consumables
- Embryo culture media (Day 1–5) and incubation
- Blastocyst grading and selection
- Embryo transfer — procedure and ultrasound guidance
- Luteal phase support medications post-transfer
- Vitrification (freeze-preservation) of surplus embryos — charged separately
- Advanced add-ons (IMSI / PICSI / PGT-A / ERA) — discussed and quoted on indication only.
Frequently Asked Questions
Is ICSI better than standard IVF in all cases?
No — ICSI is significantly superior to standard IVF specifically in male factor infertility cases, or whenever natural fertilisation is unlikely to succeed. For couples with a normal semen analysis where male factor is not a concern, standard IVF (conventional insemination) achieves comparable fertilisation rates with lower technical intervention. Dr. Pranay Shah will advise based on your specific semen analysis and clinical history — not as a routine default.
Are ICSI babies at higher risk of birth defects?
Large population studies show that ICSI babies have a marginally higher risk of certain chromosomal abnormalities compared to naturally conceived children — primarily because some male infertility conditions have a genetic component that can be transmitted. The absolute increase in risk is very small. For patients where this is a concern (particularly with azoospermia or severe teratospermia), PGT-A (preimplantation genetic testing) of embryos before transfer is available and can significantly reduce the risk of transferring chromosomally abnormal embryos. We discuss this with every patient for whom it is relevant.
What is the difference between ICSI and IMSI?
ICSI selects and injects sperm at 200–400× magnification, assessing basic shape and motility. IMSI performs the same injection but selects sperm after examination at 6,000–10,000× magnification — revealing internal nuclear defects (vacuoles) that are completely invisible at standard ICSI magnification. IMSI is recommended when ICSI alone has not produced expected outcomes, when morphology is severely abnormal, or when recurrent embryo quality problems suggest deeper sperm nuclear issues.
My husband has azoospermia. Can ICSI still help us?
Yes — in many cases. If the azoospermia is obstructive (a blockage problem), sperm is almost always successfully retrieved via PESA or TESE, and ICSI is performed with these retrieved sperm. If the azoospermia is non-obstructive (a production problem), Micro-TESE identifies viable sperm in approximately 40–60% of cases. When sperm is found, ICSI success rates are comparable to those with ejaculated sperm. A complete evaluation — karyotype, Y-chromosome microdeletion testing, hormonal profile — is recommended before proceeding.
How long does the actual ICSI injection procedure take?
The laboratory ICSI procedure itself — the actual injection of each egg — takes approximately 30–60 seconds per egg. For a typical cycle yielding 8–12 mature eggs, the entire ICSI session takes approximately 1–2 hours. This is performed on the morning of egg retrieval. Neither the male nor female partner is present in the laboratory during this procedure.
Is ICSI included in the standard IVF package at Wellspring?
ICSI is itemised separately from the basic IVF cycle cost because it involves significant additional embryologist time, specialised micromanipulation equipment, and technical expertise beyond standard IVF. Your complete itemised cost breakdown — including ICSI, culture media, and all laboratory charges — is provided in full at your consultation with Dr. Pranay Shah. We operate a strict no-hidden-costs philosophy.
What is the ICSI cost in Ahmedabad at Wellspring IVF?
A complete, itemised quotation is provided at your consultation. For an overview of our IVF and ICSI pricing, visit our IVF cost guide on our Master Hub, or call our team directly at +91 9099946050.
Related Conditions & Treatments
Male Infertility Is Not the End of Fatherhood
Related Insights & Articles
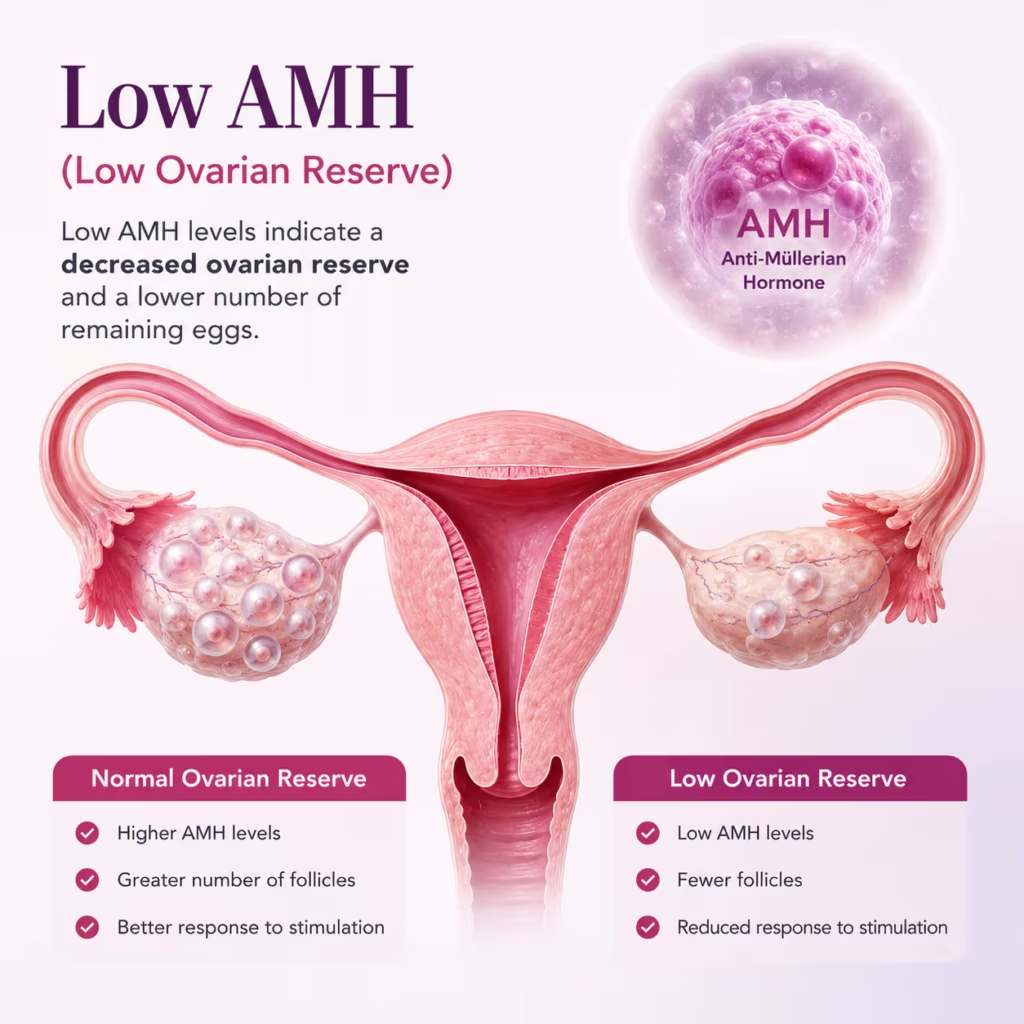
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026