What ERA measures
Frozen Embryo Transfer (FET) & Endometrial Preparation in Ahmedabad
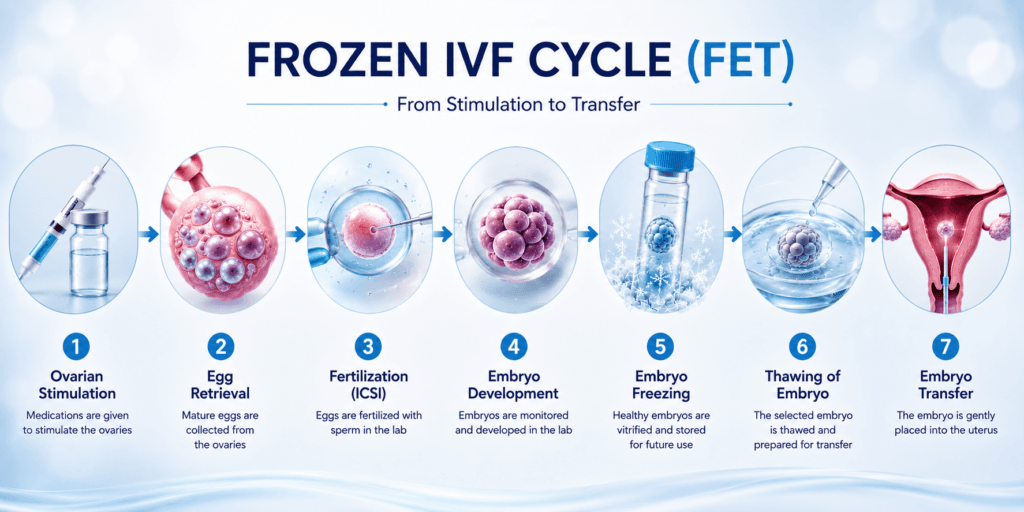
Frozen Embryo Transfer (FET) at Wellspring IVF Ahmedabad prepares a dedicated, carefully synchronised uterine lining before transferring a vitrified embryo. Modern vitrification achieves 98%+ survival on warming, and for selected patients FET is not the backup option. It is the better option.
Request a Free Callback
Your information is completely safe and confidential. By submitting, you agree to be contacted about your enquiry.
Frozen Embryo Transfer (FET) in Ahmedabad — Perfecting the Soil Before Planting the Seed
One of the most common fears about IVF:
“If they freeze the embryo, will it survive? Will it be damaged? Is a frozen embryo less likely to result in a baby than a fresh one?”
These concerns are understandable — and the science answers them clearly. Modern vitrification — the flash-freezing technology used at Wellspring IVF — achieves a 98%+ embryo survival rate on warming. A vitrified embryo is not a compromised embryo. It is an embryo in suspended animation — genetically identical, biologically unchanged, waiting to resume development the moment it is warmed. The ice crystal damage that destroyed embryos with old slow-freeze technology is eliminated by vitrification’s ultra-rapid cooling rate.
But the bigger picture goes beyond survival rates. FET is not simply a backup plan for when a fresh transfer cannot happen. For specific patient groups, FET produces better — not just equivalent — outcomes than fresh transfer. The reason is biology: ovarian stimulation hormones affect the endometrium.
When the embryo and the uterine lining are developing simultaneously in the same stimulated cycle, they are sometimes out of synchrony. In a FET cycle, the endometrium is prepared separately — in its own dedicated, hormone-controlled cycle — with the sole objective of building the most receptive lining possible before the embryo is introduced. Perfecting the soil before planting the seed.
At Wellspring IVF, Dr. Pranay Shah selects between natural cycle FET and medicated FET based on your specific hormonal profile and ovulatory pattern. He uses ERA (Endometrial Receptivity Analysis) for recurrent implantation failure cases to identify the exact window of implantation. And every FET cycle begins with a complete endometrial assessment — because the lining that receives the embryo matters as much as the embryo itself.
98%+ Embryo Survival on Warming
Vitrification — ultra-rapid flash-freezing — has made embryo freezing one of the most reliable steps in the entire IVF process. The fear of ‘frozen embryo damage’ belongs to the era of slow-freeze — a technology no longer used at specialist IVF centres. Wellspring IVF uses vitrification exclusively.
Frozen Embryo Transfer — At a Glance
| Key Aspect | Details & Clinical Approach |
|---|---|
| What Is FET | A frozen embryo — created and cryopreserved from a previous IVF stimulation cycle — is thawed and transferred to the uterus in a separate, dedicated cycle. |
| Vitrification Survival Rate | 98%+ embryo survival rate with modern vitrification (flash-freezing). Slow-freeze survival: 70–80%. Wellspring uses vitrification exclusively. |
| Total FET Cycle Duration | 3–5 weeks for endometrial preparation + transfer. No egg stimulation injections in this cycle. |
| Two Protocol Options | Natural Cycle FET: ovulation-timed transfer. Medicated FET: oestrogen + progesterone controlled preparation. |
| The Core Advantage | Endometrium prepared in a dedicated, unstimulated cycle — fully synchronised with the embryo. No OHSS risk. Progesterone not a variable. |
| Best Candidates | High responders (OHSS risk), elevated progesterone on trigger day, PGT-A cycles, recurrent implantation failure, freeze-all strategy, second baby from banked embryos. |
| Success Rate | 50–65% per transfer for good-quality vitrified blastocysts. Equivalent to or better than fresh in matched patient groups. |
| Key Science | Stimulation hormones can impair endometrial receptivity. A FET cycle removes this interference — the endometrium is built optimally without ovarian stimulation. |
| Embryo Grading on Thaw | Embryo re-graded after warming. Transfer proceeds only if the embryo meets quality threshold. No viable embryo = cycle cancelled (rare with vitrification). |
| ERA Testing | Endometrial Receptivity Analysis (ERA) available for recurrent implantation failure — identifies the precise window of implantation. |
| Consultation | 📞 9099946050 | FET protocol discussed at post-cycle review or new patient consultation. |
Vitrification — Why Frozen Embryos Are No Longer a Compromise
Vitrification is the scientific breakthrough that transformed embryo freezing from a high-risk procedure into one of the most reliable steps in the IVF process. Understanding what it does — and why it replaced slow-freeze — removes the fear of freezing.
Vitrification Explained — The Science in Plain Language
Vitrification Explained — The Science in Plain Language
The problem vitrification solved
he original slow-freeze process cooled embryos gradually over 2–4 hours. During this process, water molecules inside the embryo’s cells had time to form ice crystals. Ice crystals have sharp, angular structures — they physically rupture cell membranes and organelles. Result: many embryos survived freezing but were damaged. Slow-freeze survival rates: 70–80%. Post-thaw embryo quality was often reduced. Implantation rates with thawed slow-freeze embryos were lower than with fresh embryos.
What vitrification does instead
Vitrification cools the embryo at an extraordinary rate: approximately 15,000°C per minute — compared to slow-freeze’s 1–2°C per minute. At this speed, water molecules have no time to form ice crystals. Instead, the cellular water solidifies into a glass-like (vitreous) amorphous state — smooth, structureless, no sharp edges. Cell membranes are intact. Organelles undamaged. Genetic material completely preserved. The embryo is in perfect suspended animation.
The cryoprotectant solution
Before vitrification, embryos are briefly exposed to a cryoprotectant solution that replaces cellular water with a glass-forming solvent. This further prevents ice crystal formation during cooling. The cryoprotectant concentration and equilibration time are protocol-critical steps performed by our embryologist.
Vitrification survival rates at Wellspring IVF
98%+ of vitrified blastocysts survive the warming process intact at Wellspring IVF. This means: if you have 4 vitrified blastocysts, you can expect all 4 to survive warming and be assessed for transfer. A warmed embryo that collapses (fails to re-expand) or shows significant degeneration is rare — and when it happens, Dr. Shah’s team communicates this before the transfer appointment.
Embryo re-grading after warming
After warming, the embryo is re-assessed under the microscope. A fully expanded, high-grade blastocyst that was vitrified at Grade 5AA typically re-expands to the same grade within 2–4 hours of warming. Re-grading confirms quality before transfer. Transfer is cancelled only if the embryo fails to recover — an outcome that is rare with vitrification.
Storage duration — does time in the freezer affect quality?
No — vitrified embryos do not age or deteriorate in storage. The cryogenic state is biologically static. A blastocyst stored for 5 years has the same developmental potential as one stored for 5 months. This is validated by clinical data: large studies show no decline in live birth rate with increasing storage time. Healthy babies have been born from embryos stored for 10+ years.
| Feature | Vitrification (Used at Wellspring IVF) | Slow-Freeze (Outdated method) |
|---|---|---|
| Cooling speed | ~15,000°C per minute | 1–2°C per minute |
| Ice crystal formation | None — glass-like vitreous state | Extensive — damages membranes |
| Blastocyst survival rate | 98%+ | 70–80% |
| Post-thaw quality | Equivalent to pre-freeze in 95%+ cases | Often reduced — fragmentation |
| Implantation rate with thawed embryo | Equivalent to fresh in matched groups | Lower than fresh |
| Used at Wellspring IVF | Yes — exclusively | No — retired |
Who Is FET Best For? — The Clinical Indications
FET is not just the ‘backup’ when a fresh transfer fails. For specific patient groups, it is clinically the better first choice. Here is the complete framework:
Wellspring IVF — Treatments | IVF Hub | Frozen Embryo Transfer
| Patient Scenario | Why FET Gives Better Outcome | Why Fresh Transfer Would Be Suboptimal |
|---|---|---|
| High Responder (>15 follicles, PCOS, high AFC) | No OHSS risk. No hCG exposure to aggravate response. Endometrium prepared when oestrogen is normal, not elevated 10×. | High OHSS risk. Stimulated endometrium under extreme oestrogen load. High miscarriage risk in OHSS-affected cycle. |
| Elevated Progesterone on Trigger Day (>1.5 ng/mL) | FET cycle uses controlled progesterone supplementation — embryo-endometrium synchrony is re-established from scratch. | Premature luteinisation advances endometrial secretory phase — embryo and lining are out of sync. Significantly reduced implantation. |
| PGT-A Cycle (Genetic Testing Planned) | Genetic lab results take 2–3 weeks. Only euploid embryos transferred. FET is the only option — fresh transfer is biologically impossible. | Impossible — embryo must be biopsied, result awaited, then thawed. |
| Recurrent Implantation Failure (RIF) | Dedicated endometrial preparation cycle. ERA testing to find exact window of implantation. Optimised timing with progesterone. | Stimulation-affected endometrium is the suspected cause of prior failures — repeating fresh transfer does not address the problem. |
| Thin Endometrium During Stimulation | Medicated FET uses escalating oestrogen to build lining optimally. Hysteroscopy can be performed between cycles if structural cause found. | Transferring into a thin lining (<7mm) in a fresh cycle has poor prognosis. |
| Freeze-All Strategy (Surplus Quality Embryos) | Vitrified blastocysts available for multiple future transfers. Avoids repeat stimulation cycles. More cost-efficient per baby. | Fresh transfer uses one embryo; freeze-all preserves the full cohort for sequential transfer opportunities. |
| Second Baby — Existing Frozen Embryos | No new stimulation cycle needed. FET uses banked embryos. Significantly lower cost, time, and physical burden than a new cycle. | Full stimulation cycle at higher cost and with increased risks when suitable frozen embryos already exist. |
| Post-OHSS Recovery | Once OHSS resolves (typically 4–6 weeks), FET proceeds safely. No ovarian stimulation re-exposure. Endometrium fully recovered. | OHSS itself, or residual ovarian changes, make fresh transfer unsafe. |
Endometrial Preparation — Building the Perfect Lining
The endometrium is the most important variable in a FET cycle. The embryo is already of known quality — it was vitrified at a specific grade. What FET adds is the ability to control the uterine environment completely, without the interference of ovarian stimulation. Endometrial preparation is the whole point of FET — and it is where Dr. Shah's individualised approach delivers its greatest advantage.
Thickness — minimum 7mm, target 8–12mm
The endometrium must reach at least 7mm thickness measured by transvaginal ultrasound. The target is 8–12mm. Below 7mm: significantly reduced implantation rates. Above 12mm: not associated with better outcomes and may indicate other pathology. Thickness is monitored at each scan during preparation and is the primary metric for readiness to proceed.
Pattern — trilaminar (triple-line) appearance
On transvaginal ultrasound, a receptive endometrium shows three distinct echogenic layers — the classic ‘triple line’ pattern. This pattern indicates adequate glandular development and stromal organisation — the architecture the embryo needs to implant into. A homogeneous (non-trilaminar) or thin pattern at the expected time: Dr. Shah investigates before proceeding to transfer.
Progesterone timing — synchrony with the embryo
Progesterone initiates the secretory phase of the endometrial cycle — transforming the receptive lining into the implantation window. The embryo must arrive at the endometrium during the window of implantation (WOI) — approximately 5 days after progesterone start (Day P+5). Mis-timing by even 12 hours can affect implantation. This is why ERA testing exists — to identify the exact WOI for individual patients.
Watch Our Video on Why Frozen embryo transfer is Better Approach
Learn how Frozen embryo transfer works, when it may be recommended, and what couples can expect during the process.
What You Will Learn
Learn the difference between fresh and frozen embryo transfer and how each may affect IVF success.
- Fresh vs frozen embryo transfer basics
- Frozen IVF success and timing
- When frozen embryo transfer is recommended
- Embryo freezing and IVF treatment process
Natural Cycle FET vs Medicated FET — Which Protocol Is Right for You?
Two principal approaches to endometrial preparation. Dr. Shah selects based on your ovulatory pattern, hormone profile, and cycle regularity:
| Factor | Natural Cycle FET | Medicated / Artificial Cycle FET |
|---|---|---|
| How it works | Relies on natural ovulation — monitors LH surge, times transfer to natural progesterone | External oestrogen builds lining; progesterone added after lining confirmed ready |
| Best for | Regular, predictable ovulatory cycles. Normal AMH, normal FSH, regular periods | Anovulatory PCOS, irregular cycles, previous poor natural cycle response |
| Medications required | Minimal — LH surge monitoring + progesterone support only | Oestradiol valerate tablets/patches, progesterone pessaries (essential) |
| Monitoring scans | 3–4 scans to track dominant follicle + LH surge timing | 2–3 scans for lining assessment + progesterone start timing |
| Progesterone control | Natural corpus luteum provides progesterone — less controllable | External progesterone supplementation — completely controlled timing |
| Cycle cancellation risk | Higher — premature LH surge or ovulation before scan can cancel cycle | Lower — ovulation suppressed; progesterone start is fully controlled |
| Endometrial control | Less predictable — dependent on natural oestrogen production | Fully controlled oestrogen dose allows dose-adjustment if lining is thin |
| ERA compatibility | Yes — ERA biopsy timed to natural progesterone exposure | Yes — ERA biopsy timed to progesterone supplementation start |
| Success rate evidence | Equivalent to medicated in regular ovulators — some studies favour natural | Equivalent in matched groups; preferred for irregular cycles |
| Dr. Shah’s first choice | Regular ovulatory cycle, patient preference for minimal medication | PCOS, irregular cycle, previous natural cycle cancellation |
Modified Natural Cycle FET: A third approach combining both methods: natural ovulation is used (avoiding oestrogen injections) but a low-dose hCG injection is given at the time of LH surge to support the corpus luteum — and progesterone supplementation is added from the day after ovulation. This provides the natural endometrial environment with the security of supported luteal phase. Dr. Shah uses modified natural cycle FET in patients with good ovulatory function who have had suboptimal progesterone in previous natural cycle attempts.
The FET Cycle — Step-by-Step Timeline (Medicated Protocol)
DAY 1–2
Baseline
Menstrual Cycle Baseline Assessment
- Transvaginal ultrasound: confirm quiet ovaries, no residual cysts from previous cycle
- Uterine cavity assessment — rule out polyps, fibroid recurrence, adhesions before proceeding
- Blood tests: Day 2 LH, FSH, Estradiol, Progesterone — confirm suppressed baseline
- Previous embryo inventory confirmed: number, grade, vitrification date reviewed with embryologist
- Oestradiol valerate tablets or patches started: Day 1 or 2 of period
DAYS 1–10
Lining Build
Oestrogen Phase — Building the Endometrium
- Oestradiol valerate (Progynova) 2mg BD increasing to 2mg TID or higher if lining slow
- No injections in this phase — oral tablets or transdermal patches
- Patient avoids strenuous exercise, alcohol during lining preparation
- Monitoring scan at approximately Day 10–12: endometrial thickness, trilaminar pattern
- Target: ≥8mm trilaminar endometrium before progesterone is added
- If thin lining at first scan: dose increased, additional scan scheduled 3–5 days later
DAY 10–14
Lining Check
Endometrial Assessment Scan
- Transvaginal scan: precise measurement of endometrial thickness (three-layer measurement)
- Trilaminar pattern confirmed: all three layers must be visible
- Serum oestradiol and progesterone levels: confirms hormonal environment is ready
- Endometrium ≥8mm, trilaminar, progesterone suppressed: progesterone start scheduled
- Thin endometrium (failure to reach 7mm despite maximum oestrogen): cycle postponed, investigation planned (Doppler, hysteroscopy if structural cause suspected)
DAY 14–16
Progesterone
Progesterone Start Opening the Window
- Progesterone pessaries (Crinone 8% gel or Utrogestan 200mg) started: BD or TID vaginally
- This is ‘Day P+0’ — the start of the window of implantation countdown
- The endometrium begins secretory transformation — from receptive to implantation-ready
- Day P+5 (5 days after progesterone start): Day 5 blastocyst transfer scheduled
- Day P+3 (3 days after start): Day 3 cleavage embryo transfer (if Day 3 embryo frozen)
- Oestrogen tablets continued throughout — do not stop
DAY P+4
Embryo Thaw
Embryo Warming — Vitrification Reversal
- Embryologist removes vitrified blastocyst from liquid nitrogen storage
- Warming protocol: rapid rehydration in graded cryoprotectant solutions over 1–2 hours
- Embryo assessed under microscope: re-expansion, ICM quality, trophectoderm appearance
- Full survival and re-expansion: proceed to transfer (scheduled next morning)
- Partial survival: Dr. Shah contacted — decision to proceed or use alternative embryo made
- Survival rate at Wellspring IVF: 98%+ of vitrified blastocysts fully survive warming
- Couple notified of embryo status on warming day — before they travel for transfer
DAY P+5
Transfer
Frozen Embryo Transfer The Main Event
- Patient arrives with comfortably full bladder — aids ultrasound visualisation
- No sedation, no anaesthesia — completely comfortable outpatient procedure
- Embryo loaded in culture medium droplet in a soft catheter
- Abdominal ultrasound guides precise catheter placement in upper uterine cavity
- Embryo deposited 1–2cm from fundus — the optimal implantation zone
- Procedure duration: 5–10 minutes. Mild cramping is normal
- Embryologist confirms embryo has been transferred from the catheter (flashback check)
- Rest for 30–45 minutes. Light activity from the same evening. Work resumable next day
- Progesterone and oestrogen supplementation continues without interruption
DAY P+5 to P+19
2-Week Wait
Luteal Support During the Wait
- Continue progesterone pessaries: BD or TID exactly as prescribed — do not skip
- Continue oestradiol tablets — do not stop without Dr. Shah’s instruction
- If on LMWH (Clexane) for APS/thrombophilia: continue daily injection
- Mild spotting: normal and does not predict failure — do not stop medications
- Avoid: NSAIDs (ibuprofen, diclofenac), hot baths, saunas, vigorous exercise, alcohol
- WhatsApp access to the Wellspring IVF team throughout the wait — questions welcome
- Home urine test: wait for the blood beta-hCG for definitive result
DAY P+19
RESULT
Beta-hCG Blood Test — Pregnancy Confirmation
- Serum beta-hCG: 14 days after embryo transfer. The definitive pregnancy test
- Positive: progesterone and oestrogen support continued. First ultrasound at 6–7 weeks
- Negative: Dr. Shah consultation within 48 hours — cycle review, next embryo or protocol
- Borderline result (5–25 mIU/mL): repeat in 48 hours — doubling time confirms viability
- Remaining vitrified embryos: preserved for subsequent FET attempts — no new stimulation
- If second FET planned: next menstrual cycle start, then new preparation cycle begins
ERA Testing — For Recurrent Implantation Failure
The Endometrial Receptivity Analysis (ERA) test is offered at Wellspring IVF for patients with recurrent implantation failure — where good-quality embryos have been transferred multiple times without establishing a pregnancy.<
ERA analyses the endometrial gene expression profile at the time of the intended transfer. Using a small biopsy of the endometrial lining taken at Day P+5, next-generation sequencing identifies whether the endometrium is in its window of implantation (WOI) at the standard transfer time — or whether the WOI is displaced (pre-receptive or post-receptive). Approximately 25–30% of recurrent implantation failure patients have a displaced WOI — they are transferring at the wrong time.
For patients with a displaced WOI, ERA provides the exact adjustment needed: '+12 hours progesterone' or '+24 hours' or 'Day P+6 instead of Day P+5.' Subsequent FET cycles use the ERA-guided personalised transfer time. Published data: ERA-guided transfers improve implantation rates in recurrent implantation failure by approximately 25–30%.
Three or more failed FET cycles with good-quality blastocysts and normal endometrium. Two or more failed transfers where the embryo quality was excellent (5AA/6AA). Recurrent implantation failure after PGT-A euploid transfers. ERA is not necessary for first-cycle FET — the standard transfer timing is correct for the majority of patients.
A mock medicated FET cycle is performed without an embryo. At Day P+5 (standard transfer time), an endometrial biopsy is taken. The sample is sent to a specialist genomics laboratory. Results in approximately 2–3 weeks. The actual FET with an embryo follows in the next cycle, timed to the ERA-guided pET.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah
Director & Chief Fertility Consultant

Divyesh Bhalodia
Senior Embryologist

Urmi Chauhan
Clinical Embryologist
What Our Patients Say
Real stories from real families who trusted us with their fertility journey

Ketan B.
2 months ago
I visited many doctors before, but this doctor was the one who correctly identified my issue and provided the right treatment. I finally started seeing real results after consulting them. Very knowledgeable, attentive, and professional. Highly recommended.

vibha R.
2 months ago
Heartfelt thanks to the entire team of Wellspring Hospital. After feeling disappointed and losing hope at many places, coming here was the best decision.
A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕
A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

Kanal G.
4 months ago
Some doctors treat symptoms. Rare ones treat the human being sitting in front of them.
He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.
He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Kul C.
6 months ago
Dr Shah is highly knowledgeable, through and dedicated. He explained every step of the process in simple terms, ensuring we were informed and comfortable. The entire team and staff are very kind and caring.
Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"
Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"

chandresh T.
6 months ago
We had a great experience with Wellspring. Dr Pranay Shah is a very good person and possess the good knowledge. His guidance and treatment helped us fulfill our wishes. The hospital staff is also very kind and supportive. I strongly recommend Wellspring.

Ruchita S.
8 months ago
I want to express my heartfelt gratitude to Dr. Pranay Shah and the team at Wellspring IVF & Women’s Hospital. This journey is never easy, but Dr. Shah made me feel comfortable, cared for, and fully supported throughout the IVF process. Thank you

Mohamed I.
8 months ago
Our hearts are overflowing with gratitude and joy as we reflect on our incredible journey to parenthood, made possible by the extraordinary care and expertise of your team. The IVF process was, at times, daunting and exhausting, but your unwavering support, compassion, and professionalism helped us remain hopeful through every step. From the very first consultation to the celebratory moment when we learned our treatment was successful, we felt respected, understood, and truly cared for.Thank you for believing in us, never giving up, and guiding us through every challenge with warmth, patience, and encouragement. Your personalized guidance, gentle approach, and positive outlook gave us strength, and your medical skill brought our dream to life. We are forever grateful for your remarkable ability to merge empathy and science, giving hope to couples like us.
Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Read all our verified Google reviews or share your own experience
FET After OHSS — The Safe Pathway for High Responders
Ovarian Hyperstimulation Syndrome (OHSS) in a stimulation cycle is the clearest medical indication for a freeze-all strategy. Dr. Shah’s approach:
When OHSS occurs during stimulation:
All embryos are vitrified. No fresh transfer is performed. Administering hCG for a fresh transfer in an OHSS cycle would dramatically worsen the condition — hCG is the principal driver of OHSS severity. The pregnancy’s own hCG production would then sustain and intensify the syndrome for weeks. This is why fresh transfer in a high-risk OHSS cycle is contraindicated.
Recovery timeline before FET:
- Mild-moderate OHSS: resolves spontaneously in 10–14 days. FET can proceed in the next menstrual cycle — approximately 4–6 weeks after retrieval.
- Severe OHSS (hospitalisation): full resolution may take 3–6 weeks. Dr. Shah assesses ovarian appearance by ultrasound before clearing for FET preparation. No FET is started until ovaries are back to baseline size and all symptoms resolved.
OHSS and FET success:
Importantly, OHSS does not damage the embryos — they are safely vitrified before OHSS develops. A patient who experienced severe OHSS but has four excellent blastocysts vitrified has exactly the same embryo quality as a patient with no OHSS. The FET success rate is not reduced by having had OHSS. The recovery period is temporary. The embryos are waiting, unchanged.
“The question I get asked most about FET is: ‘Does freezing hurt the embryo?’ And my answer is always: with vitrification, the embryo we transfer is biologically identical to the one we froze. It did not age. It did not degrade. What we gained by waiting is a completely clean, prepared endometrium — built specifically to receive it, in its own dedicated cycle, without any of the hormonal noise from stimulation. For the right patient, the frozen embryo transfer is not the second choice. It is the better choice.”
Ready to Plan Your FET Cycle?
Dr. Shah reviews your frozen embryo inventory, selects natural or medicated protocol, and maps out a personalised FET preparation plan at your consultation.
Book Your Consultation
Call Us Now!
09099946050Frequently Asked Questions
Common questions on FET timing, embryo survival, natural versus medicated preparation, and fresh versus frozen decisions.
Ask a QuestionWhat is the survival rate of frozen embryos at Wellspring IVF?
Using vitrification (flash-freezing), 98%+ of blastocysts fully survive the warming process at Wellspring IVF. This is the established outcome for modern vitrification at specialist centres. The old fear of ‘frozen embryo damage’ applied to slow-freeze technology — a method no longer used at Wellspring IVF. Embryos that do not survive warming (rare with vitrification) are identified on the morning of the transfer appointment — and you are informed before you travel.
Is a frozen embryo transfer as successful as a fresh transfer?
For the right patient group: yes — and sometimes more successful. Large randomised studies show FET success rates are equivalent to fresh in normal responders. In high responders (PCOS, elevated oestrogen at trigger), FET is significantly better — because the endometrium is prepared in a dedicated, unstimulated cycle without the progesterone elevation that impairs fresh endometrial receptivity. For PGT-A cycles (chromosomally normal embryos), FET is the only option. Wellspring IVF FET success rate: 50–65% per transfer for good-quality vitrified blastocysts.
How long do I have to wait between egg retrieval and a FET cycle?
Typically one complete menstrual cycle — approximately 4–6 weeks after egg retrieval. This allows the ovaries to return to baseline, hormone levels to normalise, and the endometrium to shed and regenerate. In OHSS recovery cases, Dr. Shah waits until all symptoms have fully resolved and the ovaries appear quiet on ultrasound before starting FET preparation — this may take 6–10 weeks in severe cases.
Can frozen embryos be stored indefinitely?
Vitrified embryos do not deteriorate in storage — the cryogenic state is biologically static. Embryos stored for 5+ years show the same implantation rates as those stored for 6 months in published clinical data. Under India’s ART (Regulation) Act 2021, embryo storage duration and consent are regulated. At Wellspring IVF, embryo storage is handled in compliance with the Act. Annual storage fees apply. Storage consent is renewed periodically. Dr. Shah discusses long-term embryo storage plans at your post-cycle review.
What if my embryo doesn't survive the thaw?
With vitrification, this is rare — the survival rate at Wellspring IVF is 98%+. If the embryo does not survive warming (degeneration or collapse), you are notified on the morning of the scheduled transfer — before you travel. If you have additional vitrified embryos, they can be warmed for a rescheduled transfer. If no further embryos are available, Dr. Shah discusses next steps — which may include a new stimulation cycle. Non-survival of an embryo on thaw is never assumed without direct microscopic assessment on the warming day.
What medications will I need to take during a medicated FET cycle, and are there side effects?
In a medicated FET cycle, your ovaries are kept at rest while we rebuild your uterine lining using external hormones. You will primary use two medications:
Oestradiol Valerate: Started on Day 1 or 2 of your period (either as oral tablets like Progynova or transdermal patches) to thicken the endometrium. Side effects are usually mild and can include temporary bloating, breast tenderness, or slight mood fluctuations.
Progesterone Support: Started once the lining is confirmed ready (≥8mm and trilaminar). This is typically administered as vaginal pessaries or gels (like Crinone or Utrogestan), and occasionally via subcutaneous injections. Progesterone can cause symptoms that mimic early pregnancy—such as mild fatigue, bloating, or breast heaviness.
Unlike a fresh IVF cycle, there are no painful ovarian stimulation injections, and the risk of Ovarian Hyperstimulation Syndrome (OHSS) is entirely eliminated.
Do I need complete bed rest after a Frozen Embryo Transfer? What are the lifestyle restrictions?
No, complete bed rest is not required and is actually not recommended by modern reproductive medicine. Clinical studies show that lying perfectly still does not improve implantation rates; your uterus is a muscular organ that safely holds the embryo in place.
What you should do instead:
Activity: You will rest at Wellspring IVF for about 30 to 45 minutes immediately following the 5–10 minute procedure. After that, you can return to light, routine daily activities. You can safely return to desk work the very next day.
What to avoid: During the “two-week wait,” avoid strenuous high-impact exercise, heavy lifting (over 15kg), hot baths, saunas, and swimming pools (to prevent vaginal infection from the water). Keep walking and moving naturally to maintain good blood circulation to the pelvis.
Related Treatment & Condition Pages
IVF Treatment Hub — Master Guide
Fresh IVF Cycle & Embryo Transfer
Embryo Freezing (Vitrification) Full Guide
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026

Your Frozen Embryo Is Waiting. The Perfect Lining Is the Final Step.
98%+ survival. 50–65% success rate per transfer. A dedicated endometrial preparation cycle built for exactly one purpose.
Dr. Pranay Shah will review your embryo inventory, select your preparation protocol, and take you through every step of the FET journey at your consultation.
Dr. Pranay Shah will review your embryo inventory, select your preparation protocol, and take you through every step of the FET journey at your consultation.