IVF Protocol for Low AMH in Ahmedabad
Request a Free Callback
📋IVF Protocol For Low AMH at Wellspring – Details at Glance
- Why standard high-dose IVF often backfires in low AMH patients — the biology explained
- Mini-IVF (Mild Stimulation Protocol) — full clinical explanation, indications, and embryo pooling strategy
- DuoStim (Dual Stimulation) — retrieving eggs TWICE in one menstrual cycle
- Embryo Pooling — the strategy that changes everything for low AMH
- Pre-cycle optimisation — DHEA, CoQ10, and lifestyle factors that improve egg quality
- Choosing the right protocol for your specific AMH level
- Success rates — honest, evidence-based expectations
- The bridge to Donor Egg IVF — when and how we have that conversation
Maximising Every Single Egg — Advanced Strategies for Poor Ovarian Reserve
“Your AMH Is Low.”
Those three words carry enormous emotional weight. In one sentence, they can make a woman feel as if her body has failed her, as if IVF will not work, as if motherhood with her own eggs is no longer possible.
At Wellspring IVF & Women’s Hospital, we challenge the idea that low AMH automatically means IVF will fail. Low AMH does not mean zero eggs. It means we must use protocols that are biologically suited to women with fewer follicles, instead of forcing a normal-reserve IVF approach onto a poor-reserve ovary.
Protocol logic, not generic IVF advice for Low AMH IVF success
Mini-IVF · DuoStim · Embryo Pooling · Your Own Eggs, First
- Why standard high-dose IVF often backfires in low AMH patients — the biology explained
- Mini-IVF (Mild Stimulation Protocol) — full clinical explanation, indications, and embryo pooling strategy
- DuoStim (Dual Stimulation) — retrieving eggs TWICE in one menstrual cycle
- Embryo Pooling — the strategy that changes everything for low AMH
- Pre-cycle optimisation — DHEA, CoQ10, and lifestyle factors that improve egg quality
- Choosing the right protocol for your specific AMH level
- Success rates — honest, evidence-based expectations
- The bridge to Donor Egg IVF — when and how we have that conversation
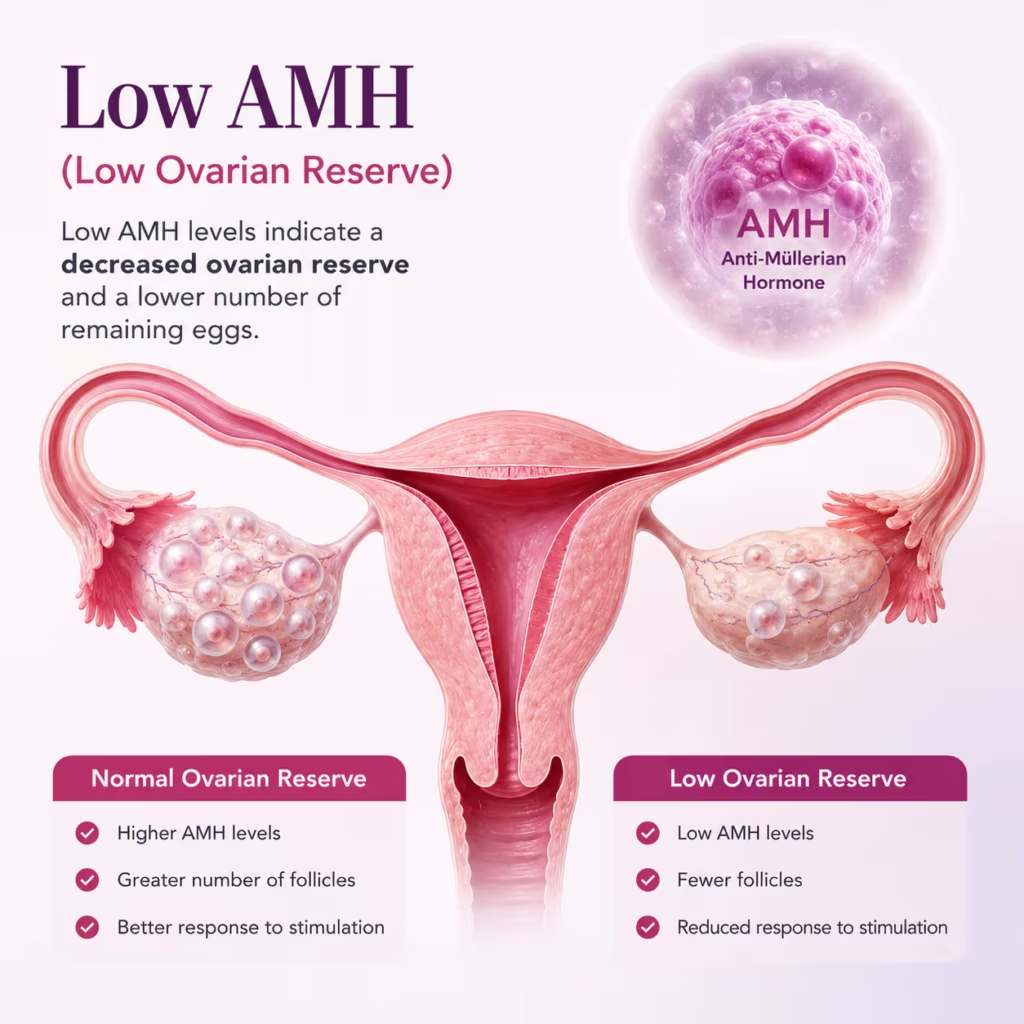
Understanding AMH - The Ovarian Reserve Marker That Changes Everything
Anti-Mullerian Hormone is produced by the small antral follicles in the ovaries. It is the most reliable single blood test for estimating ovarian reserve because it reflects egg quantity more consistently across the menstrual cycle than many other hormones.re is the complete comparison:
Critical distinction: AMH measures quantity, not quality.
A woman with low AMH may still have eggs of excellent quality, especially if she is under 35. The challenge is that fewer follicles are available for stimulation, which usually means fewer eggs, fewer embryos, and a lower chance of success from any one cycle. That is exactly why protocol choice matters so much.
| AMH Level (ng/mL) | Clinical Interpretation | Protocol Direction at Wellspring IVF |
|---|---|---|
| Above 1.5 | Normal / Good Reserve | Standard IVF protocol |
| 1.0 – 1.5 | Low-Normal / Borderline | Modified protocol with close monitoring |
| 0.5 – 1.0 | Low Ovarian Reserve | Mini-IVF or modified antagonist protocol |
| 0.1 – 0.5 | Very Low Reserve | Mini-IVF or DuoStim with embryo pooling |
| Below 0.1 | Critically Low | All options discussed, including Natural Cycle IVF and donor eggs |
The high FSH and low AMH combination
Many low AMH patients also have an elevated Day-2 or Day-3 FSH. This tells us the pituitary is working harder to recruit follicles because the ovarian reserve is diminished. It does not mean IVF cannot work. It means conventional high-dose stimulation is often the wrong biological match.
Watch Our Low AMH Managment Video
Learn how low AMH affects fertility and what treatment options may help improve pregnancy chances.
What You Will Learn
Learn how low AMH Managment with proper protocol improve pregnancy outcome
- Low AMH and ovarian reserve basics
- Pregnancy chances with low AMH
- IVF options in low AMH cases
- Fertility treatment and egg quality factors
Why Conventional High-Dose IVF Often Fails Low AMH Patients
The common logic behind conventional IVF is simple: more stimulation should mean more eggs. In women with low AMH and poor ovarian reserve, that logic frequently breaks down because the ovary does not have additional follicles available to recruit just because the medication dose is higher.
The biology of ovarian non-response
- In women with low AMH, there are simply fewer follicles available to respond to stimulation. The follicles that are present may already be sensitised or may respond poorly to high FSH doses.
- Beyond a certain threshold, administering more FSH does not recruit more follicles — because the additional follicles are not there to recruit. The ovary has already been pushed to its maximum.
- What high-dose stimulation in low AMH patients often achieves: identical or fewer eggs retrieved compared to a gentler approach, but with significantly higher medication costs, greater physical discomfort, and — critically — higher risk of cycle cancellation.
Key Research Finding — Evidence for Mild Stimulation in Poor Responders
Multiple randomised controlled trials and systematic reviews — including studies published in Fertility & Sterility and Human Reproduction — demonstrate that in poor ovarian responders (POR):
- Mild stimulation protocols produce similar numbers of mature eggs as high-dose protocols
- Fewer cancelled cycles with mild stimulation
- Lower medication burden and significantly reduced cost
- Comparable cumulative live birth rates when embryo pooling is employed
- Dr. Pranay Shah’s clinical approach at Wellspring IVF is grounded in this evidence base — not in the convenience of a high-dose default.
Advanced IVF Protocols for Low AMH at Wellspring
There is no single correct protocol for low AMH. Dr. Pranay Shah selects the most appropriate strategy based on your AMH level, AFC, age, FSH, prior IVF response, and how much time pressure exists in your case.
Mini-IVF Mild Stimulation
Mild Stimulation Protocol — Working With Your Ovaries, Not Against Them
Mini-IVF — also called Minimal Stimulation IVF or Natural-Modified IVF — represents a fundamentally different philosophical approach to ovarian stimulation. Instead of forcing the ovaries to produce as many eggs as possible, we work with the ovaries’ natural monthly rhythm, collecting fewer but potentially higher-quality eggs with significantly less medication.
How Mini-IVF Works:
- Stimulation: Low-dose oral medication (Clomiphene Citrate or Letrozole) often combined with a small dose of FSH injections (50–75 IU/day vs 225+ IU in conventional IVF). Only the most naturally dominant follicles are recruited.
- Expected Egg Yield: Typically 1–4 mature eggs per cycle (vs 8–15 in a conventional IVF cycle for a normal responder).
- Embryo Quality: Because mild stimulation minimises hormonal disruption and selects the most naturally competitive follicles, egg and resulting embryo quality is often preserved or superior compared to high-dose stimulation.
- Cycle Cancellation Rate: Very low — working with follicles that naturally wish to develop, the cycle is less likely to be abandoned due to poor response.
- Physical Comfort: Significantly reduced injection burden, virtually no risk of OHSS, and a gentler overall treatment experience.
Who Is Mini-IVF Best Suited For?
- AMH 0.1–0.8 ng/mL — very low to low ovarian reserve
- AFC 1–5 (Antral Follicle Count) — few resting follicles on baseline scan
- Women who have responded poorly or not at all to previous high-dose IVF cycles
- Elevated Day-3 FSH (> 12–15 IU/L) — the ‘loud pituitary’ pattern
- Women who prefer a lower-medication approach with multiple sequential cycles
- Women where premature ovarian insufficiency (POI) is a clinical concern
The Embryo Pooling Strategy — The Game-Changer for Low AMH
The most powerful application of Mini-IVF in low AMH patients is not a single cycle — it is a series of 2–4 Mini-IVF cycles run over 2–4 months, with all resulting embryos vitrified (frozen) from each cycle. Once a sufficient number of embryos has been accumulated, the best-quality embryo is selected for Frozen Embryo Transfer (FET).
Mini-IVF Cycle 1 — Stimulate → Retrieve → Freeze All Embryos The first Mini-IVF cycle is performed with mild stimulation. Typically 1–4 eggs are retrieved. After ICSI fertilisation, resulting embryos are cultured to Day 3 or Day 5 (blastocyst). All suitable embryos are vitrified (frozen) — no fresh transfer is performed at this stage. The goal is embryo banking, not immediate transfer. |
Mini-IVF Cycle 2 — Repeat — Add to the Embryo Bank After one menstrual cycle of rest, a second Mini-IVF cycle is performed using the same or a slightly modified protocol based on Cycle 1 response. Resulting embryos are again frozen and added to the existing bank. The cumulative embryo pool is now larger than any single high-dose cycle might have produced in a poor responder. |
Mini-IVF Cycle 3–4 (If Needed) — Continue Until Milestone Target Is Reached Dr. Shah sets clear milestone targets at the outset: typically 2–4 good-quality blastocysts banked before a transfer is attempted. In some patients, 2 cycles yield sufficient embryos. In others, 3–4 cycles build the pool. The decision to proceed to transfer is made when the pool is clinically adequate — not on an arbitrary timeline. |
Frozen Embryo Transfer (FET) — Transfer When the Conditions Are Optimal Once the embryo pool is established, the best-quality embryo is selected for FET in a well-prepared endometrial cycle. This is timed independently of stimulation — when the uterine lining is ideal. FET success rates in a well-prepared cycle are comparable to or better than fresh transfer, and the uterine environment is significantly calmer and more receptive. |
Why Embryo Pooling Changes the Probability Calculation
- A single Mini-IVF cycle may yield 1–2 embryos — giving a limited transfer probability from one attempt.
- A pool of 3–4 embryos from sequential cycles gives multiple transfer opportunities — dramatically improving the cumulative live birth probability over 12–16 weeks of sequential cycles.
- This is not a slower path to pregnancy — it is a smarter use of your biological resources when each individual cycle cannot be expected to produce the same yield as a normal responder.
DuoStim Dual Stimulation
Dual Stimulation — Two Egg Retrievals in One Menstrual Cycle
DuoStim is a more intensive strategy for patients with critically low AMH who require maximum egg yield in the shortest possible time. It exploits a biological discovery from the last decade: luteal phase follicles are recruitable — the ovaries can be stimulated TWICE in a single menstrual cycle, producing two separate egg retrieval procedures approximately 10–14 days apart.
How DuoStim Works:
- Stimulation 1 — Follicular Phase (Days 2–12): Standard Mini-IVF or mild stimulation begins at the start of the cycle. Egg retrieval (OPU-1) is performed at Day 12–14 when follicles are mature.
- Stimulation 2 — Luteal Phase (Days 14–26): Immediately following OPU-1, a second stimulation cycle begins — taking advantage of the wave of luteal phase follicles that would otherwise be lost. OPU-2 is performed approximately Day 22–26.
- All embryos frozen: Embryos from BOTH retrievals are vitrified. The combined pool is then used for a subsequent FET in the next naturally prepared cycle.
- Time advantage: DuoStim effectively compresses what would be 2 monthly Mini-IVF cycles into a single month — providing a larger embryo pool faster, which is valuable when age or time pressure is a factor.
Who Is DuoStim Best Suited For?
- AMH below 0.5 ng/mL — critically low reserve where time compression is clinically important
- Women aged 38+ with low AMH — where time is a critical biological factor
- Patients who want the maximum embryo yield in the shortest possible timeframe
- Women who have already completed 2–3 Mini-IVF cycles with limited embryo accumulation
- Couples with a specific time constraint (travel, work, medical) who need faster results
DuoStim — Follicular Phase vs Luteal Phase Embryo Quality
A common concern about DuoStim is whether luteal phase eggs are of comparable quality to follicular phase eggs. Published research — including the landmark studies by Ubaldi and colleagues — has demonstrated that luteal phase oocytes produce blastocysts of comparable quality and chromosomal integrity (assessed by PGT-A) to follicular phase oocytes. This makes DuoStim not merely a quantity strategy — it is a clinically validated approach to maximising the embryo pool without compromising embryo quality.
Natural Cycle IVF
Zero Stimulation — For the Most Extreme Low AMH Cases
For women with AMH below 0.1 ng/mL and AFC of 1–2, even mild stimulation may not reliably produce additional follicles beyond the single natural dominant follicle. In these cases, Natural Cycle IVF — collecting the one egg the body naturally selects each month without any stimulation — is a valid, lower-cost alternative that eliminates the risk of poor stimulation response and cycle cancellation.
Advantages: No stimulation medications, no OHSS risk, lower cost per cycle, can be repeated monthly, and works with the body’s natural selection mechanism.
Limitations: Single egg per cycle — if that egg does not fertilise or the resulting embryo does not develop to blastocyst, the cycle yields nothing. Requires multiple cycles for embryo pooling. Higher cycle-level variability.
Best combined with: An embryo pooling approach — multiple sequential Natural Cycle IVF attempts over 3–6 months to accumulate embryos for FET.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Choosing the Right Protocol
| Comparison Factor | Mini-IVF | DuoStim |
|---|---|---|
| AMH range most suited | 0.1-0.8 ng/mL | Below 0.5 ng/mL |
| Stimulation approach | Low-dose oral plus small FSH | Two mild stimulations in one cycle |
| Retrievals per cycle | 1 per monthly cycle | 2 within one 30-35 day cycle |
| Expected eggs | 1-4 per retrieval | 2-6 combined from both OPUs |
| Time to embryo pool | 2-4 monthly cycles | 1-2 combined DuoStim cycles |
| Procedure intensity | Lower and gentler | Higher, but faster |
| Best for | Time-flexible, lower-AMH patients | Time-pressured or age 38+ |
| OHSS risk | Very low | Very low |
Talk to Dr. Shah About Cavity Optimisation
Pre-Cycle Optimisation - Improving Egg Quality Before IVF
While AMH predicts how many eggs we might expect, egg quality can still be influenced by specific pre-cycle strategies. These are not universal recommendations. They must be assessed for your body, your diagnosis, and your safety profile.
DHEA – 8 to 12 weeks before cycle
DHEA may improve follicular response and egg quality in selected poor responders, but it is not appropriate for everyone, especially those with PCOS or hormone-sensitive conditions. It should only be prescribed and monitored by Dr. Shah.
CoQ10 – Mitochondrial support
CoQ10 supports mitochondrial function inside the egg and is often discussed in poor ovarian reserve cases. Therapeutic dosing and preparation length should be individualised in consultation.
Melatonin and sleep quality
Melatonin has been explored for its antioxidant role in follicular fluid and egg protection. Sleep quality and circadian stability are also clinically relevant in real-world IVF preparation.
Lifestyle optimisation
Healthy BMI, smoking cessation, avoiding alcohol, adequate sleep, and stress management are not generic wellness talking points here. They are practical parts of protecting egg quality and making stimulation more efficient.
Important safety note on supplements
DHEA, CoQ10, and melatonin should only be taken under direct medical supervision from Dr. Pranay Shah. Self-prescribing supplements before IVF is not safe or advisable because dosing, timing, and patient suitability all need clinical assessment.
Low AMH IVF Success Rates - Evidence-Based Expectations
Success rates in low AMH IVF are among the most commonly misunderstood numbers in fertility care. At Wellspring, the goal is not inflated optimism or defensive pessimism. It is an honest probability estimate built around age, embryo quality, AMH, AFC, and treatment response.
| Patient Profile | Per-Cycle Rate | Cumulative (3 cycles) | Key Variable |
|---|---|---|---|
| Age under 35, AMH 0.5-1.0, good embryo quality | 25-35% | 55-70% | Age remains the strongest quality factor |
| Age under 35, AMH 0.1-0.5, Mini-IVF pooling | 15-25% | 40-55% | Pool size and blastocyst grade |
| Age 35-38, AMH 0.5-1.0 | 18-25% | 40-55% | Egg quality declining — PGT-A advised |
| Age 35-38, AMH 0.1-0.5, DuoStim plus pooling | 12-20% | 30-45% | DuoStim maximises pool in time-pressured cases |
| Age above 38, AMH below 0.5 | 8-15% | 20-35% | Donor egg discussion should be honest and early |
| DuoStim combined pool from both OPUs | 18-30% | 45-60% | Greater pool means more transfer opportunities |
The most important number is your personalised estimate
Age is often a more powerful predictor of egg quality and IVF success than AMH alone. A 32-year-old with AMH 0.3 may still have a better prognosis than a 41-year-old with AMH 0.8. Dr. Shah interprets AMH, age, AFC, and embryo development together, not in isolation.
The Bridge to Donor Egg IVF - An Honest Conversation, Never Rushed
At Wellspring IVF, our philosophy is Own Eggs First. Every clinically viable option to achieve a pregnancy with a patient’s own eggs is explored before donor eggs are discussed. However, being genuinely patient-centred also means having an honest, compassionate conversation when own-egg IVF is unlikely to succeed — so that couples can make an informed decision about the path forward.
When this conversation usually begins
Dr. Pranay Shah will initiate this conversation when: two or more well-managed Mini-IVF or DuoStim cycles have failed to produce viable embryos, PGT-A testing of available embryos confirms chromosomal abnormality in all assessed embryos, and age and AMH together suggest that further own-egg attempts carry very low probability with significant time cost.
| Own-Egg IVF | Donor Egg IVF |
|---|---|
| Genetic connection: yes | Genetic connection: donor egg plus partner sperm |
| Success per transfer: 12-35% depending on age and AMH | Success per transfer: 70-75% |
| Often needs multiple cycles | Single coordinated cycle is often enough |
| Time investment: often 3-6 months for pooling | Timeline depends on donor availability and cycle coordination |
| Recommended first when clinically viable | Recommended once own-egg options are genuinely exhausted |
This conversation is never rushed, never pressured, and always driven by clinical evidence and your personal values. If and when donor eggs become the right path, Wellspring IVF offers a full Donor Egg IVF programme — in full compliance with the ART (Regulation) Act 2021.
Frequently Asked Questions
Can I have a baby with my own eggs if my AMH is very low?
Yes, in many cases. AMH measures egg quantity, not quality. A younger woman with low AMH can still have good-quality eggs. The real decision depends on age, AFC, FSH, and previous IVF response, not on one AMH number alone.
Why is my doctor recommending high-dose IVF when I have low AMH? Shouldn't less stimulation be better?
Many centres still default to high-dose stimulation even for poor responders. Published research consistently shows that mild stimulation can achieve comparable or better outcomes in poor responders with lower medication burden, fewer cancelled cycles, and strong cumulative results when embryo pooling is used.
What is the difference between Mini-IVF and DuoStim? Which is better for me?
Mini-IVF uses gentle stimulation across multiple separate monthly cycles. DuoStim performs two stimulations and egg retrievals within a single menstrual cycle. DuoStim is faster, Mini-IVF is gentler and more spread out. The right choice depends on AMH level, age, time constraints, and previous response.
How many Mini-IVF cycles should I plan for?
Most embryo pooling plans are built around 2-4 cycles before transfer. Some patients reach a meaningful embryo pool in 2 cycles, while others need 3-4 cycles to build enough transfer opportunities.
Is DHEA safe to take before IVF for low AMH?
DHEA can benefit selected patients, but it is not safe or appropriate for everyone and should never be self-administered. Dr. Shah should decide whether it fits your case, the dose, and the duration.
What happens if Mini-IVF or DuoStim does not produce usable embryos?
If 2-3 well-managed cycles do not produce viable embryos, the next conversation may include protocol variation, Natural Cycle IVF, or moving to Donor Egg IVF. That discussion should be compassionate, evidence-based, and never rushed.
Will my child be genetically mine if I use my own eggs with Mini-IVF?
Absolutely. If Mini-IVF or DuoStim uses your own eggs, the resulting child carries your genetic material and your partner’s. The protocol changes stimulation strategy, not parentage.
Related Conditions & Treatments
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026