Fertility-Enhancing Surgery in Ahmedabad
Request a Free Callback
Medical & Compliance Note
Laparoscopy and hysteroscopy are surgical procedures performed under anaesthesia by a qualified gynaecologist. The decision to recommend either is made by Dr. Pranay Shah after clinical evaluation, review of investigations, and discussion of all options — not every patient with infertility needs surgery. Surgery is recommended only when a specific, correctable cause is identified. Any success or improvement figures on this page are population-level data from peer-reviewed literature; individual outcomes vary with age, diagnosis, anatomy, and clinical history. No guaranteed outcome is implied (ASCI healthcare guidelines + medical ethics). Wellspring IVF operates in compliance with the ART (Regulation) Act 2021.

3000+
15+
Day-Care
Fertility-Enhancing Surgery in Ahmedabad — Laparoscopy & Hysteroscopy
For many couples, the obstacle to pregnancy is not a mystery that requires IVF — it is a physical, correctable cause. A polyp sitting in the uterine cavity. A patch of endometriosis distorting the pelvis. A fibroid pressing on the cavity. A uterine septum present since birth. Fix the cause, and natural conception — or a subsequent IVF cycle — has a far better chance.
That is what fertility-enhancing surgery does. At Wellspring IVF & Women’s Hospital, Dr. Pranay Shah uses two minimally invasive, day-care procedures — laparoscopy (keyhole surgery of the pelvis) and hysteroscopy (cavity surgery through the cervix, with no incision at all) — to diagnose and treat these causes. With 15+ years in minimally invasive surgery and 350+ hysteroscopic procedures, his approach is conservative and precise: operate only when there is a clear, correctable reason, and do it in a way that protects your fertility.
This page explains what each surgery is, which conditions it treats, and — crucially — when surgery should come before IVF and when IVF should be the direct route. If surgery is recommended for you, you will be told exactly why. The answer is one call away: 📞 9099946050.
Surgery at Wellspring IVF — In Three Numbers │ 3000+ Hysteroscopic Procedures │ 15+ Yrs Minimally Invasive Surgery │ Day-Care Most Patients Home Same Day
Watch Our Video on Role of Diagnostic Laparoscopy & Hysteroscopy Before IVF
Learn when diagnostic laparoscopy and hysteroscopy may be recommended before IVF to identify hidden fertility problems.
What You Will Learn
Understand the role of laparoscopy and hysteroscopy in fertility evaluation and treatment planning.
- Laparoscopy and hysteroscopy basics
- Detecting hidden fertility issues
- When these procedures are needed
- Their role before IVF treatment
What Is Fertility-Enhancing Surgery?
Fertility-enhancing surgery refers to minimally invasive procedures that diagnose and correct structural or anatomical causes of infertility — problems in the uterus, fallopian tubes, ovaries, or pelvis that prevent conception or implantation. Unlike open surgery, these procedures use either keyhole incisions or a natural opening (the cervix), so recovery is fast and most are performed as day-care.
The aim is specific: remove or repair the thing that is standing in the way. Sometimes this restores the ability to conceive naturally. Sometimes it prepares the body for a more successful IVF cycle — for example, by optimising the uterine cavity before an embryo transfer. Surgery is not a treatment everyone needs; it is recommended only when an assessment finds a correctable cause.
At Wellspring, fertility surgery is built on two complementary procedures, often used together in a single sitting for a complete picture of both the pelvis and the uterine cavity.
Laparoscopy vs Hysteroscopy — What Is the Difference?
This is the most common point of confusion, and the distinction is simple once seen clearly: laparoscopy looks at the outside (the pelvis), hysteroscopy looks at the inside (the uterine cavity). One uses tiny abdominal keyhole incisions; the other uses no incision at all, entering through the cervix.
| Factor | Laparoscopy | Hysteroscopy |
|---|---|---|
| What it examines/treats | The pelvis — ovaries, tubes, outer uterus, pelvic cavity | The inside of the uterus — the endometrial cavity |
| Route | Keyhole incisions in the abdomen (usually 2–3 small cuts) | Through the cervix — no incision at all |
| Main conditions | Endometriosis, ovarian cysts, fibroids, blocked/damaged tubes, pelvic adhesions | Polyps, submucosal fibroids, uterine septum, intrauterine adhesions (Asherman’s) |
| Anaesthesia | General anaesthesia | Short/general anaesthesia — often very brief |
| Typical recovery | A few days to about a week | Usually 1–2 days |
| Role before IVF | Treats pelvic disease (e.g. endometriosis, hydrosalpinx) that lowers IVF success | Optimises the cavity so an embryo can implant |
| Wellspring page | Laparoscopy for Infertility → | Hysteroscopy for Infertility → |
Laparoscopy — Keyhole Surgery of the Pelvis
Laparoscopy is keyhole surgery performed through 2–3 small abdominal incisions, using a camera and fine instruments. It lets Dr. Shah both see and treat pelvic causes of infertility in the same sitting — removing endometriosis deposits, ovarian cysts, or fibroids; freeing adhesions; and assessing or repairing the fallopian tubes. Because the incisions are tiny, recovery is far quicker than open surgery. Read the complete laparoscopy guide →
Hysteroscopy — Cavity Surgery with No Incision
Hysteroscopy passes a thin camera through the cervix into the uterus — there is no cut on the body at all. It is the definitive way to inspect the cavity and correct anything that could prevent implantation: polyps, a submucosal fibroid, a uterine septum, or scar tissue (Asherman’s syndrome). It is the key “implantation-optimisation” procedure, frequently performed before IVF or after failed cycles. Dr. Shah has performed 350+ hysteroscopic procedures. Read the complete hysteroscopy guide →
Combined Laparoscopy + Hysteroscopy in One Sitting
In many infertility cases, Dr. Shah performs both procedures together under a single anaesthesia — laparoscopy to assess and treat the pelvis, hysteroscopy to assess and treat the cavity. This gives a complete structural evaluation, treats everything correctable at once, and means a single recovery rather than two. It is one of the most efficient diagnostic-and-therapeutic steps in fertility care for the right patient.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Conditions Treated by Fertility Surgery
Surgery is matched to the cause. The table below maps the most common conditions to the procedure that addresses them — each links to its full condition guide.
| Condition | Procedure | What Surgery Achieves |
|---|---|---|
| Endometriosis | Laparoscopy | Removes/ablates deposits, frees adhesions, restores pelvic anatomy |
| Uterine fibroids | Laparoscopy or Hysteroscopy | Removes fibroids distorting the cavity or pressing on it (myomectomy) |
| Uterine polyps | Hysteroscopy | Removes polyps from the cavity to improve implantation |
| Blocked / damaged fallopian tubes | Laparoscopy | Assesses tubes; treats hydrosalpinx before IVF; selected tubal repair |
| Adenomyosis | Laparoscopy (selected) | Surgical management in selected cases as part of a fertility plan |
| Uterine septum | Hysteroscopy | Septum resection to restore a normal cavity — important for recurrent miscarriage |
| Intrauterine adhesions (Asherman’s) | Hysteroscopy | Divides scar tissue to restore a healthy endometrial cavity |
| Ovarian cysts | Laparoscopy | Removes cysts while preserving ovarian tissue and reserve |
Surgery vs IVF — and Surgery Before IVF: Dr. Shah’s Decision Framework
When surgery comes first (correct, then conceive or transfer)
- A uterine septum, significant polyp, or submucosal fibroid distorting the cavity — corrected by hysteroscopy before any embryo transfer, because implantation rates improve markedly once the cavity is normal.
- A hydrosalpinx (a fluid-filled, blocked tube) — best treated laparoscopically before IVF, because the fluid is known to reduce embryo implantation.
- Intrauterine adhesions (Asherman’s) — divided hysteroscopically to restore a receptive endometrium before transfer.
- Symptomatic or anatomy-distorting endometriosis in a younger patient with time — laparoscopic treatment may restore natural fertility and improve subsequent IVF.
When IVF is the direct route (bypass rather than operate)
- Both tubes blocked with no other surgical target — IVF bypasses the tubes entirely; tubal surgery is rarely worthwhile.
- Advanced maternal age or low ovarian reserve where time is the scarce resource — extensive surgery that delays treatment can do more harm than good.
- Severe male factor — the limiting factor is sperm, not anatomy; IVF/ICSI is the answer.
- Small, asymptomatic findings that do not distort the cavity — often best left alone rather than operated on.
Why Sequence Matters
Operating on something that does not need operating delays treatment and carries unnecessary risk. Skipping a simple corrective surgery — and transferring good embryos into a cavity with a polyp or septum — wastes those embryos and the cycle. The skill is in reading which is which. At Wellspring, surgery is recommended only when correcting the cause genuinely improves your chance of a baby — and never as a routine step before IVF.
Start Your Fertility Journey Today
The Day-Care Surgical Experience
Both procedures at Wellspring are designed around minimally invasive, day-care principles: small or no incisions, short anaesthesia, and same-day discharge in most cases. You arrive in the morning, the procedure is performed in our day-care theatre, you recover for a few hours, and you go home the same day. Hysteroscopy recovery is typically 1–2 days; keyhole laparoscopy a few days to a week. Dr. Shah performs the surgery personally and reviews the findings and next steps with you directly — not through a report passed between teams.
Wondering Whether You Need Surgery — or Can Go Straight to IVF? That single question is worth a consultation. Dr. Shah reviews your scans and history, identifies whether a correctable cause is present, and tells you honestly whether surgery, IVF, or surgery-then-IVF gives you the best chance. 📞 Call 9099946050
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Why Wellspring IVF for Fertility Surgery
Dr. Shah performs the surgery personally. Your laparoscopy or hysteroscopy is performed by Dr. Pranay Shah himself, with 15+ years in minimally invasive surgery and 350+ hysteroscopic procedures — not delegated to a rotating team. Consistency of the operating hand matters.
Surgery and IVF under one roof. Because Wellspring is a single fertility centre with its own theatre and embryology lab, surgery is planned as part of your overall fertility strategy — not as an isolated procedure. The surgeon and the IVF consultant are the same person, so the plan is seamless.
A conservative, fertility-protecting approach. Surgery is recommended only when a correctable cause is found, and performed to protect ovarian reserve and the uterine cavity. The goal is always your fertility — not the procedure for its own sake.
Combined sitting where appropriate. When both the pelvis and cavity need assessment, Dr. Shah can perform laparoscopy and hysteroscopy together under one anaesthesia — one recovery, complete evaluation.
Cavity optimisation before IVF. For patients heading into IVF, correcting the cavity first (a polyp, septum, or adhesion) is one of the most reliable ways to improve implantation — and it is built into the Wellspring IVF pathway.
“Patients are often surprised when I recommend a small surgery before IVF — and equally surprised when I advise against surgery they were told they needed. Both decisions come from the same principle: I operate only when fixing the cause genuinely improves your chance of a baby. A polyp or a septum in the cavity can quietly defeat good embryos; correcting it first changes everything. But operating on a blocked tube when IVF will simply bypass it only costs you time. My job is to tell you which situation you are in — honestly.” — Dr. Pranay Shah, MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
Frequently Asked Questions
Do I need surgery before IVF?
Not everyone does — surgery before IVF is recommended only when a specific, correctable problem is found that would otherwise reduce IVF success. The clearest examples are a uterine septum, a significant polyp or submucosal fibroid distorting the cavity, intrauterine adhesions, or a hydrosalpinx (fluid-filled blocked tube). Correcting these first markedly improves implantation. If no such cause is present, IVF proceeds directly. Dr. Pranay Shah assesses your cavity and pelvis and explains exactly whether surgery is indicated for your case — it is never a routine step.
What is the difference between laparoscopy and hysteroscopy?
Laparoscopy is keyhole surgery of the pelvis, performed through 2–3 small abdominal incisions, used to treat endometriosis, ovarian cysts, fibroids, pelvic adhesions, and tubal problems. Hysteroscopy examines and treats the inside of the uterus through the cervix, with no incision at all, used for polyps, a uterine septum, submucosal fibroids, and scar tissue. In short: laparoscopy addresses the outside (the pelvis), hysteroscopy the inside (the cavity). Both are minimally invasive and frequently performed together in a single sitting.
Is fertility surgery painful, and how long is recovery?
Both procedures are performed under anaesthesia, so there is no pain during surgery. Hysteroscopy involves no incision and recovery is usually 1–2 days, often with only mild cramping. Keyhole laparoscopy involves small incisions and recovery is typically a few days to about a week, with some shoulder or abdominal discomfort for a short period. Most patients are discharged the same day. Dr. Shah gives you specific post-operative guidance based on the exact procedure performed.
Will surgery help me conceive naturally, or do I still need IVF afterwards?
It depends on the cause. For some patients — for example, younger women with treatable endometriosis or a corrected uterine septum — surgery can restore the ability to conceive naturally. For others, surgery is a step that improves the success of a subsequent IVF cycle rather than replacing it. Dr. Shah will tell you, based on your full picture (age, reserve, partner’s sperm, and the specific finding), whether surgery is likely to enable natural conception or is best paired with IVF.
When is surgery recommended over IVF, and when is IVF recommended directly?
Surgery is favoured when there is a correctable cause whose treatment improves your chance — a cavity abnormality before transfer, a hydrosalpinx, or symptomatic endometriosis in a younger patient with time. IVF is the direct route when both tubes are blocked with no other target, when age or low ovarian reserve makes time critical, or when the limiting factor is severe male infertility. Often the answer is surgery then IVF. Getting the sequence right is exactly what the consultation determines.
Are laparoscopy and hysteroscopy day-care procedures?
Yes — both are performed as minimally invasive, day-care surgery in most cases. You arrive in the morning, the procedure is done in our day-care theatre under anaesthesia, you recover for a few hours, and you go home the same day. There is no large incision and no prolonged hospital stay for routine fertility procedures. Dr. Shah reviews the findings and your next steps with you before discharge.
Who performs the surgery at Wellspring?
All fertility surgery at Wellspring is performed personally by Dr. Pranay Shah, Director and Chief Fertility Consultant, who has 15+ years of experience in minimally invasive gynaecological surgery and has performed 350+ hysteroscopic procedures. Because he is also the IVF consultant, surgery is planned as part of your overall fertility strategy, with seamless continuity from operation to IVF.
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
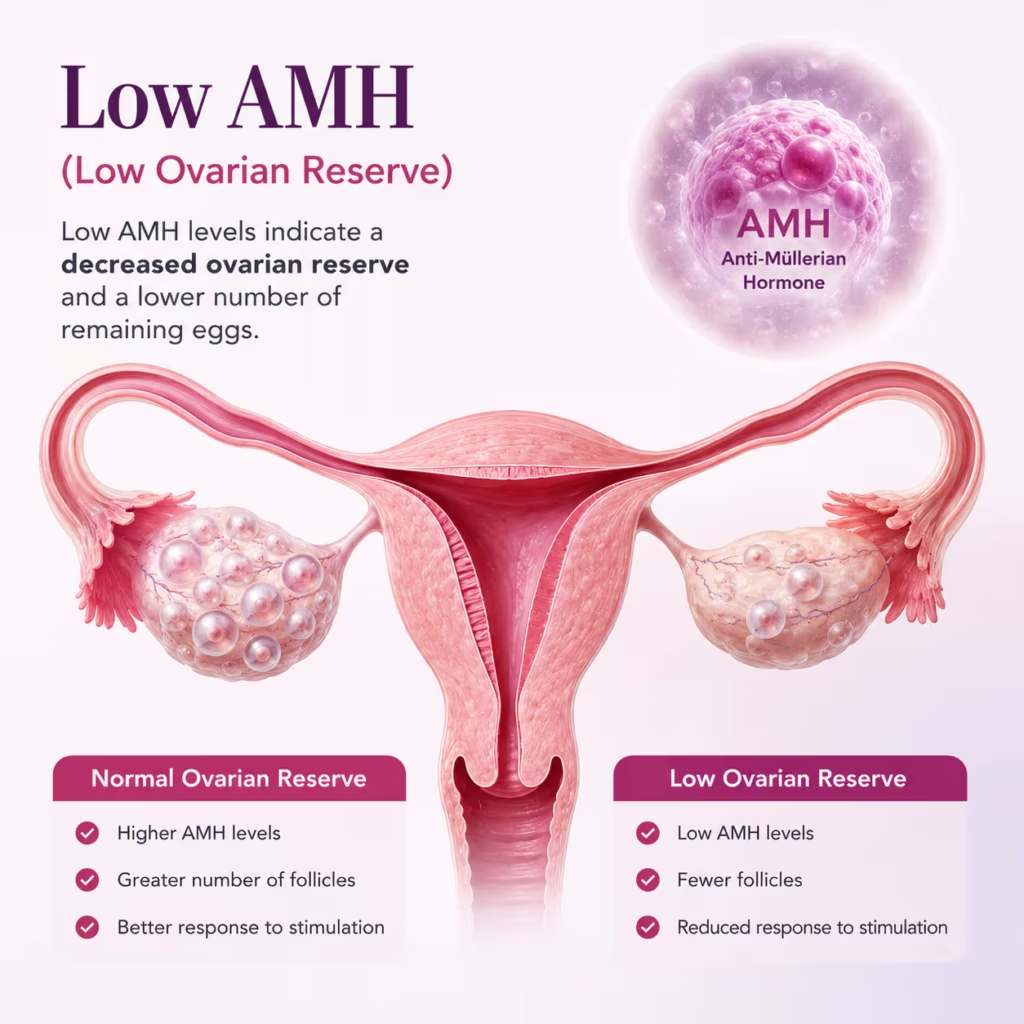
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026