PGS & PGD Genetic Testing (PGT-A / PGT-M) in Ahmedabad
Request a Free Callback
At Wellspring IVF, Dr. Pranay Shah uses Next-Generation Sequencing (NGS) to screen all 46 chromosomes before transfer — ensuring every embryo we transfer is biologically verified to have the highest chance of a healthy pregnancy.
— Dr. Pranay Shah, Director & Chief Fertility Consultant, Wellspring IVF & Women's Hospital
PGT-A vs PGT-M — Understanding the Difference
The term ‘Preimplantation Genetic Testing’ covers two different tests addressing two different clinical problems:
PGT-A (Formerly: PGS)
Full name: Preimplantation Genetic Testing for Aneuploidies
What it tests: All 46 chromosomes via NGS. Identifies euploid (normal) vs aneuploid (abnormal) embryos.
Who it is for: Women aged 35+, recurrent IVF failure, recurrent miscarriage, high sperm DNA fragmentation, prior chromosomally abnormal pregnancy.
Primary benefit: Transfer only chromosomally verified embryos — reducing miscarriage and improving live birth rates per transfer.
PGT-M (Formerly: PGD)
Full name: Preimplantation Genetic Testing for Monogenic Diseases
What it tests: A specific, pre-identified gene mutation. A custom genetic probe must be designed before the IVF cycle begins.
Who it is for: Carriers of Thalassemia, SMA, Sickle Cell, Huntington’s, BRCA1/2, Cystic Fibrosis, Fragile-X.
Primary benefit: Prevents transmission of known serious genetic disease to the child. Regulated under PCPNDT Act 1994.
PGT-A vs PGT-M — Quick Comparison
| Feature | PGT-A (PGS) | PGT-M (PGD) |
|---|---|---|
| What it tests | Chromosome number — all 46 screened | Specific inherited gene mutation |
| Technology | Next-Generation Sequencing (NGS) | Custom PCR + NGS probe design |
| Who it is for | Advanced age, recurrent failure, recurrent miscarriage | Carriers of known hereditary conditions |
| Pre-cycle preparation | Minimal — standard IVF workup | Extensive — custom probe design (4–8 weeks) |
| Biopsy timing | Day 5 Blastocyst trophectoderm biopsy | Day 5 Blastocyst trophectoderm biopsy |
| Requires freeze-all? | Yes — results take 10–21 days | Yes — mandatory FET cycle |
| Sex selection? | ILLEGAL — PCPNDT Act 1994 | ILLEGAL — PCPNDT Act 1994 |
| Primary benefit | Reduces failed transfers and miscarriage | Prevents child inheriting genetic disease |
Watch Our PGT-A Treatment Video
Learn how IUI treatment works, when it may be recommended, and what couples can expect during the process.
What You Will Learn
Learn how PGT-A/PGS-PGD helps evaluate embryo genetics and improve IVF treatment planning.
- Embryo genetic testing basics
- PGT-A and chromosome screening
- IVF failure and genetic factors
- Healthy embryo selection process
Who Should Consider PGT Testing?
1. Women of Advanced Maternal Age (35 years and above)
Egg quality declines significantly with age. By age 40, more than 60% of embryos may carry chromosomal abnormalities. PGT-A identifies the viable embryos within the cohort — saving time, cycles, and emotional resources.
2. Recurrent IVF Failure (2 or more failed transfers)
When morphologically good embryos repeatedly fail to implant, chromosomal abnormality is a primary undiagnosed cause. PGT-A determines whether the problem is genetic — before investing in another complete cycle.
3. Recurrent Pregnancy Loss (2 or more miscarriages)
Approximately 50–60% of first-trimester miscarriages result from chromosomal aneuploidy. PGT-A dramatically reduces recurrence risk by ensuring only euploid embryos are transferred.
4. Previous Chromosomally Abnormal Pregnancy
A prior pregnancy with Down Syndrome (Trisomy 21), Edwards Syndrome, Patau Syndrome, or other chromosomal conditions indicates elevated risk. PGT-A substantially reduces recurrence probability.
5. Severe Male Factor / High Sperm DNA Fragmentation
Significant sperm DNA damage (high DFI score) is associated with higher rates of chromosomal errors in embryos after fertilisation. PGT-A provides an additional verification layer.
6. Carriers of a Hereditary Genetic Disease (PGT-M)
Couples with confirmed Thalassemia, Sickle Cell, SMA, Huntington’s Disease, BRCA mutations, or other single-gene disorders should discuss PGT-M with Dr. Shah to prevent disease transmission.
Important Note: PGT does not improve egg quality or create better embryos. Its purpose is accurate selection — identifying the embryo with the highest biological probability of a healthy live birth from the embryos already available. Dr. Pranay Shah will only advise PGT when it is clinically appropriate.
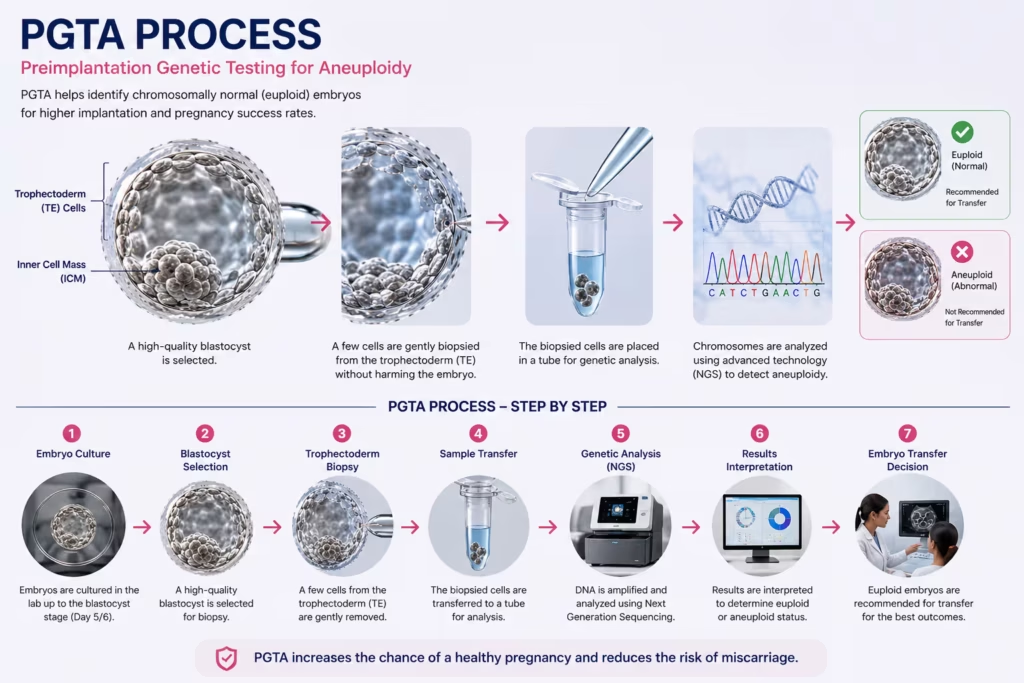
How PGT-A Works — Step-by-Step at Wellspring IVF
Step 1 — Pre-Cycle Genetic Counselling
Dr. Pranay Shah reviews your complete clinical history — age, previous IVF outcomes, miscarriage history, family genetic conditions. He confirms whether PGT-A or PGT-M is indicated and discusses realistic expectations, transparent costs, and the requirement for a freeze-all cycle.
Step 2 — IVF Stimulation and Egg Retrieval
A standard controlled ovarian stimulation protocol is followed. The goal is to retrieve an adequate number of mature eggs. Having multiple embryos is advantageous — a larger cohort increases the probability of finding at least one euploid embryo.
Step 3 — Fertilisation via ICSI and Blastocyst Culture
Eggs are fertilised using ICSI (Intracytoplasmic Sperm Injection). Embryos are cultured to the blastocyst stage (Day 5 or Day 6). Only blastocysts of adequate quality proceed to biopsy. Day 3 biopsy has been largely abandoned globally.
Step 4 — Trophectoderm Biopsy (Critical Step)
The embryologist uses a precision laser-assisted system to remove 4–6 cells from the trophectoderm — the outer layer that becomes the placenta. The inner cell mass (which forms the baby) is completely undisturbed. This procedure is safe and validated across thousands of cycles globally.
Step 5 — Freeze-All: Embryo Vitrification
Immediately after biopsy, all embryos are vitrified (flash-frozen). A fresh transfer is not possible — genetic results take 10–21 days. All embryos are stored safely until results are received.
Step 6 — Next-Generation Sequencing (NGS) Analysis
Biopsied cells are analysed at our partnered NABL-accredited genetics laboratory. NGS screens all 24 chromosome types, categorising each embryo as: Euploid (normal — suitable for transfer) | Aneuploid (abnormal — not suitable) | Mosaic (mixed — requires counselling).
Step 7 — Frozen Embryo Transfer of Verified Euploid Embryo
Once results are received, Dr. Pranay Shah personally consults the couple. In the next prepared Frozen Embryo Transfer (FET) cycle, the highest-quality euploid embryo is carefully thawed and transferred under ultrasound guidance.
Why Day 5 Biopsy — Not Day 3?
What Is a Mosaic Embryo?
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Genetic Diseases Detected by PGT-M (PGD)
| Genetic Condition | Inheritance | Relevance for Gujarat / India | |
|---|---|---|---|
| Beta-Thalassemia Major | Autosomal Recessive | One of the most prevalent inherited blood disorders in Gujarat. Carrier couples face a 25% risk of a severely affected child per pregnancy. | |
| Sickle Cell Disease | Autosomal Recessive | HBB gene mutation. High carrier frequency in tribal and certain communities across Gujarat. | |
| Huntington’s Disease | Autosomal Dominant |
| |
| BRCA1 / BRCA2 Mutations | Autosomal Dominant | Hereditary breast and ovarian cancer syndrome. PGT-M prevents passing high-risk mutations to daughters. | |
| Spinal Muscular Atrophy (SMA) | Autosomal Recessive | SMN1 gene deletion. PGT-M prevents transmission of progressive neuromuscular weakness in carrier couples. | |
| Cystic Fibrosis | Autosomal Recessive | CFTR gene mutations. PGT-M identifies unaffected embryos before transfer — preventing a severe lung and digestive disease | |
| Fragile-X Syndrome | X-Linked | FMR1 gene CGG expansion — leading genetic cause of intellectual disability. PGT-M prevents transmission. | |
| Duchenne Muscular Dystrophy | X-Linked Recessive | DMD gene mutation. Carrier mothers can use PGT-M to select unaffected embryos for transfer. |
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Is PGS/PGD the Right Step for You?
Does PGT-A Actually Improve Outcomes? — Evidence-Based Analysis
Patient Profile | Aneuploidy Rate Without PGT | Benefit of PGT-A | Dr. Shah’s Recommendation |
|---|---|---|---|
Women aged 35–37 | 40–50% of embryos aneuploid | Identifies euploid embryos; faster time-to-pregnancy | Recommended |
Women aged 38–40 | 55–65% of embryos aneuploid | Identifies the viable minority in the cohort | Strongly Recommended |
Women aged 41 and above | 70–80% of embryos aneuploid | Critical selection; informs donor egg decision | Strongly Recommended |
Recurrent implantation failure | Chromosomal cause often undetected | Reveals if genetics is the root cause | Strongly Recommended |
Recurrent miscarriage | High aneuploidy rate in embryos | Euploid transfer: 10–15% vs 25–40% miscarriage rate | Strongly Recommended |
Women under 35, first cycle, good response | 20–30% of embryos aneuploid | Marginal benefit; many euploid embryos naturally available | Not routinely recommended |
Dr. Shah’s Philosophy: ‘I do not recommend PGT-A to every patient. In a 28-year-old with good ovarian reserve and no history of failure, the cost and delay of a freeze-all cycle may not be justified. But in the right clinical context — recurrent failure, advanced age, proven miscarriage — PGT-A is one of the most powerful tools available. The decision is always personalised, never standard.’
Frequently Asked Questions
Does trophectoderm biopsy harm the embryo?
Modern Day 5 trophectoderm biopsy is considered very safe. Cells removed are from the trophectoderm (future placenta), not the inner cell mass (which forms the baby). Multiple peer-reviewed studies confirm no difference in birth defect rates between children born from biopsied versus non-biopsied embryos. Performed exclusively by senior embryologists at Wellspring IVF.
How much does PGT-A / PGS testing cost in Ahmedabad?
PGT-A costs are additional to the IVF cycle cost. The total depends on the number of embryos biopsied and the genetics laboratory. Dr. Pranay Shah provides a fully transparent cost breakdown during consultation — in line with Wellspring IVF’s No Hidden Costs philosophy. Call 9099946050 for current pricing.
Can PGT-A be done if I only have 1 or 2 embryos?
Technically yes, but this requires careful discussion. With only one or two embryos, PGT-A may reveal both are aneuploid — leaving no embryo to transfer. With a larger cohort (5+ blastocysts), PGT-A reliably identifies the best candidate. Dr. Shah will advise whether your cohort size justifies testing.
What happens if all embryos come back aneuploid?
This is emotionally difficult, but clinically important information. It confirms chromosomal quality is the core issue — and prevents multiple futile transfers or miscarriages. The pathway typically involves another stimulation cycle with a modified protocol, and if indicated, an honest consultation about donor egg options.
Is sex selection with PGD legal in India?
Absolutely not. Sex selection for non-medical reasons is a criminal offence under the PCPNDT Act 1994, punishable by imprisonment and financial penalties. Wellspring IVF will never discuss, offer, or perform any procedure for sex selection. Any such request will be firmly refused.
Does a euploid embryo guarantee pregnancy?
No. Euploid means correct chromosome number — the single largest cause of implantation failure addressed by PGT-A. However, a successful pregnancy also depends on uterine receptivity, endometrial quality, immune factors, and progesterone support. PGT-A gives each transfer the highest possible biological probability of success.
How long does PGT-M workup take before my IVF cycle?
PGT-M requires significant preparation. A custom genetic probe must be designed for your family’s mutation — typically taking 4–8 weeks before the IVF cycle can begin. Early consultation with Dr. Shah is essential if you carry a known hereditary condition.
IVF Treatment — Related Pages & Sub-Treatments
Related Insights & Articles
 Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026
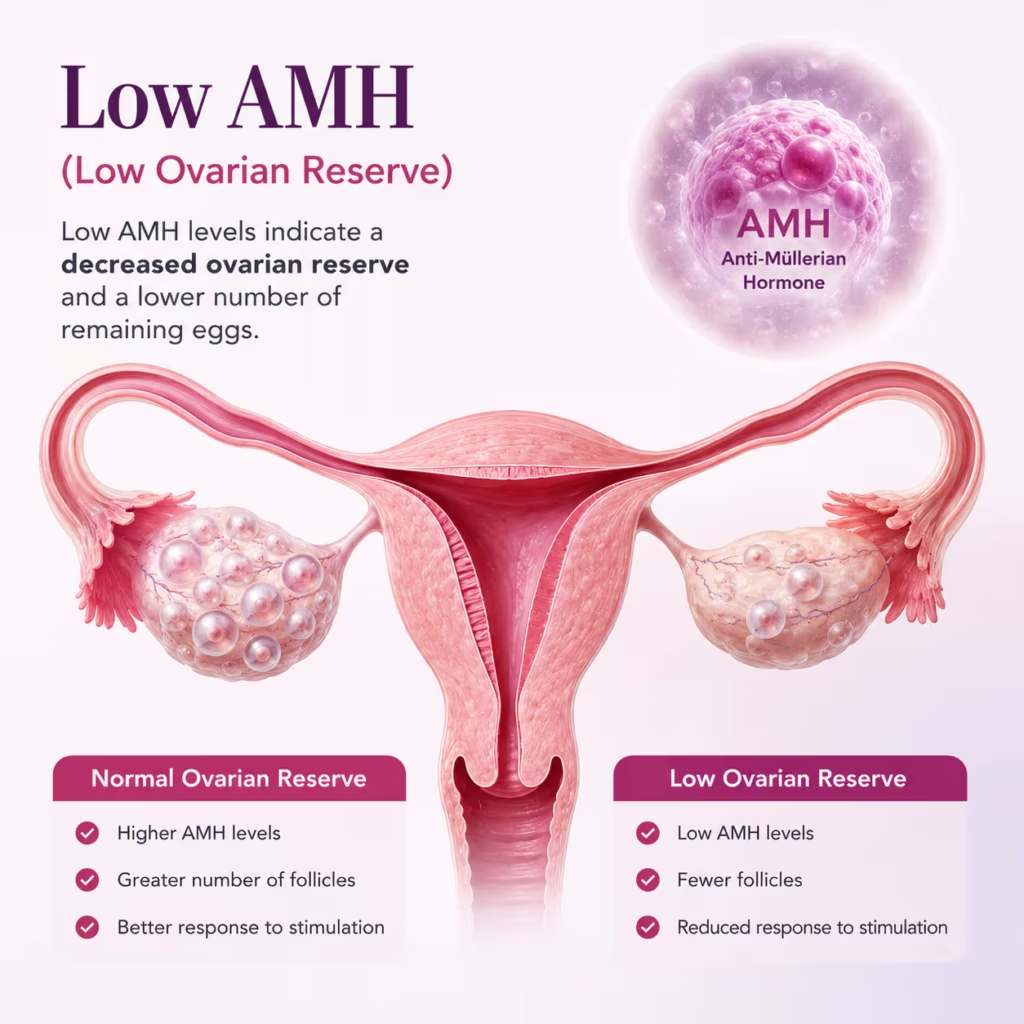
Blocked fallopian tubes can make it hard for a woman to get pregnant. But there are ways to treat this…June 11, 2026- Are you feeling worried about low AMH and IVF? You are not alone. Many women have to face the same…June 11, 2026
- Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026